
Earlier studies have demonstrated an auditory effect of lead exposure in children, but information on the effects of low chronic exposures needs to be further elucidated.
ObjectiveTo investigate the effect of low chronic exposures of the auditory system in children with a history of low blood lead levels, using an auditory electrophysiological test.
MethodsContemporary cross-sectional cohort. Study participants underwent tympanometry, pure tone and speech audiometry, transient evoked otoacoustic emissions, and brainstem auditory evoked potentials, with blood lead monitoring over a period of 35.5 months. The study included 130 children, with ages ranging from 18 months to 14 years, 5 months (mean age 6 years, 8 months±3 years, 2 months).
ResultsThe mean time-integrated cumulative blood lead index was 12μg/dL (SD±5.7, range: 2.433). All participants had hearing thresholds equal to or below 20dBHL and normal amplitudes of transient evoked otoacoustic emissions. No association was found between the absolute latencies of waves I, III, and V, the interpeak latencies I–III, III–V, and I–V, and the cumulative lead values.
ConclusionNo evidence of toxic effects from chronic low lead exposures was observed on the auditory function of children living in a lead contaminated area.
Estudos anteriores têm demonstrado efeitos da exposição ao chumbo no sistema auditivo em crianças, porém a exposição deste metal em níveis baixos ainda precisa ser investigada.
ObjetivoInvestigar os efeitos da exposição crônica ao chumbo no sistema auditivo de crianças com histórico de baixo nível sanguíneo de chumbo por meio de um teste eletrofisiológico.
MétodoEstudo de coorte transversal contemporânea. Foram realizados imitanciometria, audiometria tonal liminar e vocal, emissões otoacústicas evocadas transientes e potenciais evocados auditivos de tronco encefálico, com o monitoramento sanguíneo de chumbo durante um período de 35,5 meses. Participaram 130 crianças na faixa etária de 18 meses a 14 anos e 5 meses (6a8m±3a2m).
ResultadosA média estimada do índice de pumblemia foi 12μg/dL (DP±5,7). Todos os participantes apresentaram limiares auditivos iguais ou inferiores a 20 dBNA e amplitude normal das emissões otoacústicas evocadas transientes. Não foi encontrada associação entre as latências absolutas das ondas I, III e V e interpicos I-III, III-V e I-V e os valores cumulativos de chumbo.
Conclusãonão foi observada evidência de efeitos tóxicos em baixas exposições crônicas ao chumbo sobre a função auditiva de crianças que vivem em uma área contaminada por este metal.
Lead is a known neurotoxic agent that can cause serious damage to nervous tissue, particularly during development of the central nervous system, resulting in neurocognitive and neurophysiological disorders in children and adults. Both occupational and environmental sources of lead exposure constitute a public health concern.
Adverse health effects (especially in cognitive function, attention and learning) have been linked to low levels of lead in blood (<10–20μg/dL).1–5 In a review of the literature on the neurotoxicity associated with exposure of children to low levels of lead, the authors concluded that there is no safe level without neurological effects in the body (no adverse effect level), i.e., any exposure to lead is harmful to the central nervous system.6 One of the goals of Healthy People Program 2020 of the U.S. Department of Health and Human Services (DHHS) included the elimination of lead levels in blood ≥10μg/dL in children younger than 5 years of age by the year 2020.7 In Brazil, there is no policy directed toward the prevention of poisoning by environmental exposure to heavy metals and current Brazilian standards still consider 40μg/dL as the recommended biological index.8
Different types of evoked potentials and several neurobehavioral tests have been used to detect subclinical changes in individuals exposed to a range of lead levels, in order to prevent acute and/or persistent neurological disorders in exposed individuals.9 Schwartz and Otto10 suggested that the evoked potential may be the most sensitive indicator of central nervous system dysfunction in children. Evidence from studies on the effects of occupational exposure to lead on the human auditory system has been reported over the past three decades. Effects on latency and amplitude were reported in somatosensory, visual, and auditory evoked potentials, including cognitive evoked potential.11–23 However, there is no consensus: (1) on the limit and the level of lead poisoning needed to induce effects on the auditory system of children; (2) which structures or functions of the auditory system are susceptible; and (3) the most sensitive tests for the assessment of lead poisoning effects.
The first study that used brainstem auditory evoked potential (BAEP) to investigate the effects on electrophysiological recordings in children exposed to lead was performed by Otto et al.24 The results showed a significant association between the levels of blood lead (mean 28μg/dL) and the absolute latencies of waves III and V, with an increase in latency correlating with the increased levels of lead in blood. This finding suggested the effect of this metal occurs at the level of the lower brainstem in the cochlear nucleus region. However, the presence of cochlear damage was not ruled out.
Subsequent studies in children with higher exposure levels (43–72μg/dL) also described changes in BAEPs, which supported auditory system impairment, but with no consensus on which auditory system structures were affected. Some of these studies suggested peripheral lesions,13,25 while others suggested both central and peripheral dysfunctions.26 However, these findings were not confirmed in other studies,27,28 which found no significant association between lead exposure and auditory function. An exception was the paper of Holdstein et al.,13 that assessed the effects of lead levels in blood obtained from previous records. In this study, the researchers used lead levels in blood obtained at the time of the investigation as a biomarker of lead exposure.
With this in perspective, the purpose of this study was to investigate the effect of chronic exposure to lead on the auditory system of children with a history of low blood lead levels, using an electrophysiological test.
MethodsThis was a contemporary cross-sectional cohort study, approved by the Ethics Committee of the Institution, under No. 098/2009. Children living near a battery factory that caused lead contamination in the soil and river were recruited to participate in the study, due to their high risk of lead exposure. Those who had blood lead levels ≥10μg/dL were eligible for the study, a criterion based on the 1991 recommendation of the Centers for Disease Control and Prevention, which identified the blood lead level of 10μg/dL as “level of concern”.29
The study included 130 children (80 males and 50 females), aged 18 months to 14 years (mean: 6 years, 8 months±2 years 3 months). Levels of lead in the blood were evaluated longitudinally, with all participants submitted to audiological assessment. Study participants underwent an extensive clinical evaluation by a team consisting of a pediatrician, a neurologist, a dentist, and a speech therapist, and were free of any symptoms or diagnosed disease.
Monitoring of lead levels in bloodThe monitoring of lead levels in blood was conducted during a period lasting 35.5 months. Participants provided two to four blood samples, collected in heparinized tubes by the laboratory in charge following standard procedures. The analyses were performed under the control of the Municipal Health Secretariat and the city's Regional Health Division, and were all sent to the same laboratory for analysis. Samples were transported at 4°C and kept at this temperature prior to analysis. The blood lead level was obtained using atomic absorption spectrometry with graphite furnace.
The data of the original sample were used to assess eligibility, and the eligible cases, that is, the children with blood lead results ≥10μg/dL and without any associated disease, were followed for a period of 35.5 months. During this study, there were four sessions for blood collection; all participants were invited to participate in each of them, but not all did.
Audiometric screeningInitially, an otoscopic assessment was performed to exclude the presence of perforated tympanic membrane or otitis externa.
The audiometric test was performed to rule out any conductive or sensorineural hearing loss in the frequencies correlated with those of the click stimulus (500–4000Hz), with the aim of controlling interference on the results of the electrophysiological testing. The results of pure-tone audiometry were classified as normal if the hearing thresholds were ≤20dBHL, obtained with a MIDIMATE 622 clinical audiometer model and TDH-39P phones. Tympanometry was performed using GSI TympSTAR equipment, and tympanometry curves were considered normal when the static compliance was 0.3–1.3mL and the maximum compliance peak pressure was 90–100daPa, according to the protocol used in the service.
The tests were performed in a booth with acoustic treatment in accordance with the ANSI standard.30
The recording of transient evoked otoacoustic emissions (TEOAEs) was obtained in children aged 2 years, 6 months and older, using the Otodynamics ILO292 DP ECHO Research OAE System. The probe stability was always >80% and the stimulus was calibrated before each day of data collection. Criteria were the presence of TEOAE response, reproducibility of 70% or higher, and a response amplitude <3dB in the frequency band of 1500–5000Hz. The results of pure tone audiometry, TEOAE, and tympanometry were within normal clinical values, confirming the absence of sensorineural or conductive hearing loss in all participants.
BAEPsThe test was performed using a Hortmann auditory evoked potentials system in an electrically shielded sound-proof booth, with the child sitting comfortably, sleeping or with eyes closed, in order to eliminate the artifacts caused by eye movement. Disposable Kedall electrodes, model Medi-trace 200, were positioned as follows: active electrode Fz, reference electrode/earth in M1 and M2 (right and left mastoids), to record the ipsilateral BAEP. The individual electrode impedance was less than 5kΩ, and between electrodes, less than 2kΩ. The click stimulus was presented through a TDH-39 earphone at an intensity level of 80dBHL, with alternating polarity to reduce electrical artifacts, and a presentation rate of 21.1clicks/s, averaging 1000 stimuli in each collection, with bandpass filter of 30 and 3000Hz. Wave reproducibility was used to identify the presence of responses. The first ear to be tested was randomly chosen. The absolute latencies of waves I, III, V, and the values of interpeak intervals I–III, III–V, and I–V were measured in milliseconds (ms).
Statistical analysisDescriptive statistical analysis was performed by considering the components of the BAEP recorded separately in each ear, lead levels in blood, and the estimated blood lead values. Considering the lack of certainty about the cumulative effect of lead on the auditory system, i.e., its influence in the long-term, the authors decided to study the possible influence of the duration of lead poisoning on the results of the BAEPs. For that purpose, the blood lead value estimated on the day of the audiological assessment was calculated having as reference the date when the first blood sample was collected from the population. The audiological assessment was performed at different times for each participant; however, within the period of blood lead level monitoring.
During the study period, several measures were taken to prevent the children's exposure to lead, and the data confirmed that the levels of lead in blood decreased as a result of such interventions. Pearson's correlation coefficient was calculated for the response variables (absolute latencies of waves I, III, and V and values of interpeak intervals I–III, III–V, I–V) and the independent variables (age, values of lead in blood obtained from collections made, and estimated blood lead values).
Subsequently, a linear regression model was used for the right and left ears, using the absolute latency and interpeak values. Linear regression was the method used to select variables in the model, and the significance level was set at p≤0.05.
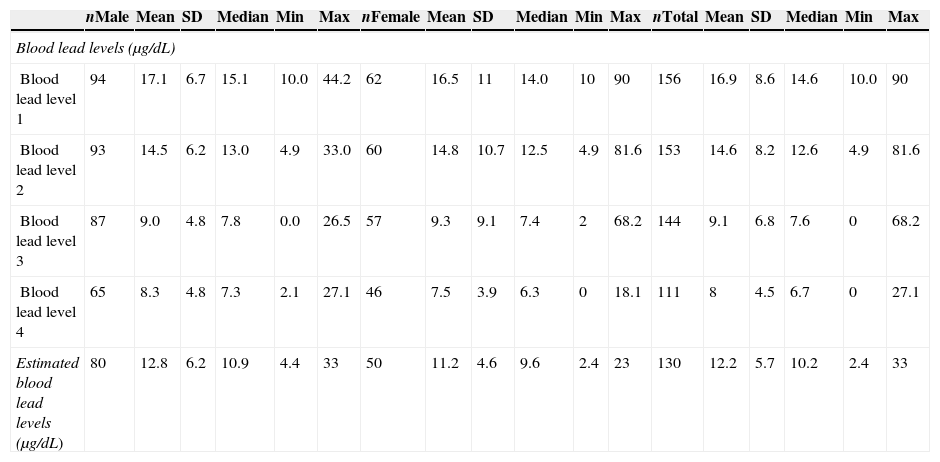
ResultsIn the present study, blood collection for the measurement of lead levels was performed four times throughout a period of 35 months; the results for each blood lead level (1st to 4th) are shown for each date of collection. The number of participants in each collection varied, despite efforts to include all participants on each occasion. The estimated blood lead level was 12.2μg/dL (±5.7μg/dL SD, ranging from 2.4 to 33μg/dL SD). Table 1 shows the results of the descriptive statistical analysis (mean, standard deviation, median, minimum, and maximum values) of lead levels in blood obtained during the period of lead level monitoring and estimated blood lead levels.
Descriptive statistics (mean, standard deviation, median, minimum, and maximum values) considering the blood lead levels obtained and estimated blood lead levels for males and females.
| nMale | Mean | SD | Median | Min | Max | nFemale | Mean | SD | Median | Min | Max | nTotal | Mean | SD | Median | Min | Max | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Blood lead levels (μg/dL) | ||||||||||||||||||
| Blood lead level 1 | 94 | 17.1 | 6.7 | 15.1 | 10.0 | 44.2 | 62 | 16.5 | 11 | 14.0 | 10 | 90 | 156 | 16.9 | 8.6 | 14.6 | 10.0 | 90 |
| Blood lead level 2 | 93 | 14.5 | 6.2 | 13.0 | 4.9 | 33.0 | 60 | 14.8 | 10.7 | 12.5 | 4.9 | 81.6 | 153 | 14.6 | 8.2 | 12.6 | 4.9 | 81.6 |
| Blood lead level 3 | 87 | 9.0 | 4.8 | 7.8 | 0.0 | 26.5 | 57 | 9.3 | 9.1 | 7.4 | 2 | 68.2 | 144 | 9.1 | 6.8 | 7.6 | 0 | 68.2 |
| Blood lead level 4 | 65 | 8.3 | 4.8 | 7.3 | 2.1 | 27.1 | 46 | 7.5 | 3.9 | 6.3 | 0 | 18.1 | 111 | 8 | 4.5 | 6.7 | 0 | 27.1 |
| Estimated blood lead levels (μg/dL) | 80 | 12.8 | 6.2 | 10.9 | 4.4 | 33 | 50 | 11.2 | 4.6 | 9.6 | 2.4 | 23 | 130 | 12.2 | 5.7 | 10.2 | 2.4 | 33 |
A strong linear correlation was found between the results of the initial lead level samples in blood and the time of audiological assessment (Pearson's r=0.78). The following variables were included in each subsequent model: latency of waves I, III, or V, age, gender, time of audiological assessment, and estimated blood lead levels on the date of the audiological assessment. To investigate the association between levels of lead in blood with the results of BAEP, the absolute latencies of waves I, III, and V were included in the model (with wave III latency adjusted for wave I latency, and wave V latency adjusted for wave III latency). The results of the initial regression of the absolute latency of wave I by ear in relation to age, gender, cumulative blood lead levels, and date of the audiological assessment were not significant.
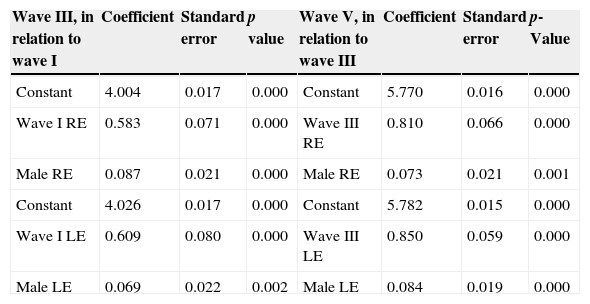
Table 2 shows the final regression model for the absolute latency of waves III and V (variables with no significant associations were not included in the table). The association between absolute latencies and gender was significant. In this study, male children had higher latencies and interpeak intervals, with a significant difference when compared to female children.
Results of the final linear regression model measuring the brainstem auditory evoked potential (absolute latency of waves III and V), right and left ears, for males compared to females.
| Wave III, in relation to wave I | Coefficient | Standard error | p value | Wave V, in relation to wave III | Coefficient | Standard error | p-Value |
|---|---|---|---|---|---|---|---|
| Constant | 4.004 | 0.017 | 0.000 | Constant | 5.770 | 0.016 | 0.000 |
| Wave I RE | 0.583 | 0.071 | 0.000 | Wave III RE | 0.810 | 0.066 | 0.000 |
| Male RE | 0.087 | 0.021 | 0.000 | Male RE | 0.073 | 0.021 | 0.001 |
| Constant | 4.026 | 0.017 | 0.000 | Constant | 5.782 | 0.015 | 0.000 |
| Wave I LE | 0.609 | 0.080 | 0.000 | Wave III LE | 0.850 | 0.059 | 0.000 |
| Male LE | 0.069 | 0.022 | 0.002 | Male LE | 0.084 | 0.019 | 0.000 |
RE, right ear; LE, left ear.
Concern about the effects of lead on health has led to several experimental and clinical studies conducted with industrial workers, adults, and children with a history of lead exposure. Lead levels in blood reflect the dynamic balance between absorption, retention, release, and elimination of the substance. In long-term exposure, this marker provides a reliable indicator of current exposure, unless the exposures vary widely, in which case the previous exposures will not be accurately reflected.
In the present study, the reduction in the blood lead levels was observed over time, and the last two samples showed that the mean level of lead in the blood of the participants was lower than 10μg/dL. The decrease in the blood lead levels in the studied children probably reflects the impact of the measures taken by the municipal government and the company responsible for the contamination of the area around the factory. Even though the study was still in progress, the participants were treated due to lead poisoning, streets and public spaces near the battery factory were paved, and the affected population received information to avoid the consumption of local products from the community garden, as well as other information related to general health.
Although studies conducted with workers exposed to lead show consistent results that indicate auditory effects, the data on the effects of environmental lead exposure on the auditory system of children are contradictory.13,25–28,31 Schwartz and Otto10 suggested that evoked potentials can provide an early indication of lead contamination when compared to behavioral procedures, but subsequent studies,27,28,31 including the present, study have failed to confirm that assertion.
The present study showed no association between low levels of lead in blood and the absolute latencies and interpeak interval values obtained in the BAEP assessment of children contaminated by lead. The regression model used in the study (which included the variables age, estimated blood lead levels, the time between audiological assessment and collection of blood, and gender of participants) showed that the only significant association was observed between the absolute latencies of waves III and V and gender (Table 2). The male children demonstrated significantly higher latencies and interpeak intervals compared to females, but the changes were not related to levels of lead in blood.
The association between the absolute latencies of BAEP and gender was expected, as the literature reports that BAEPs are affected by gender and age, due to anatomical and functional differences between genders. This finding is important considering that although some studies evaluated a control group matched to the test group in relation to gender and age, the statistical model frequently used to show the presence of a dose–effect association did not necessarily consider the influence of these independent variables. In one such study, for instance, which reported an association between auditory function and the blood lead level, a decrease in the correlation was demonstrated after the inclusion of age and gender in the statistical analysis.18
Thus, unlike the results described by other investigators,13,24–26 the present study found no association between BAEP and the cumulative blood lead level, in agreement with the results obtained by Counter et al.27,28,31 Lead levels in the present study were lower than those in the aforementioned studies. The threshold and lead poisoning level necessary to induce a neuropathology are yet to be established. In a scientific opinion of the Nordic Expert Group on the association between occupational exposure to chemicals and the incidence of hearing loss, the group defined the no-observed-adverse-effect level (NOAEL) and the lowest-observed-adverse-effect level (LOAEL) for lead, in animals and humans, specifically regarding impact on the auditory system.23 A NOAEL of 35–40μg/dL and a LOAEL of 55μg/dL in blood were identified in monkeys.
In adult humans, the effects on the central auditory system have been associated with current exposures and weighted mean life-time of lead concentrations in blood of approximately 28–57μg/dL, data obtained mainly in studies related to occupational exposures. In the present study, alterations in BAEP were observed in children living in lead-contaminated areas, with an estimated mean blood lead levels of 12.2μg/dL.
These results suggest that the BAEP was not sensitive to assess the auditory system in children with low levels of lead in blood. Neurotoxicity appears to be the predominant effect in the auditory system in the event of lead exposure (instead of ototoxicity). Considering this perspective, the recording of other evoked potentials or behavioral tests to investigate changes in central auditory processing appear to be more sensitive procedures for the early identification of lead-induced disorders, as described in the literature.
The association between lead exposure and the central auditory processing skills was investigated1 and higher lead levels in blood in the prenatal, neonatal, and postnatal periods were associated with poorer central auditory processing skills, as demonstrated by a filtered word test (screening test for auditory processing disorders [SCAN]).
However, the dichotic digits test and the auditory fusion test – revised (AFTR) were used to evaluate a sub-sample of 20 children from the present study group,32 as a feasibility study. The children contaminated by lead showed lower performance in relation to clinical normative data; however, there was no correlation between blood lead levels and auditory processing skills. The long latency auditory evoked N2 potential and cognitive P3 were also recorded in another sub-sample of 73 children.33
The N2 potential latency increased with the concentration of lead in blood (p=0.030), but no significant correlations were found between the concentrations of lead in blood and latency (p=0.821) or the amplitude of P3 potential (p=0.411). Considering that N2 potential is endogenous and is highly related to attention,34 this finding suggests that lead poisoning may be related to attention deficit, as previously reported.2 While different protocols of audiological assessment were performed in individuals exposed to solvents,35 further studies are needed to identify the ideal procedures to assess the auditory effects of lead contamination.
Evidence of effects of lead on cognition, including intelligence quotient (IQ), led the Center for Disease Control and Prevention to establish the level of lead in blood above 5μg/dL as the population-based reference for children, aiming at primary preventive intervention.29
DisclaimerMention of any company or product does not constitute endorsement by the Centers for Disease Control and Prevention (CDC), National Institute for Occupational Safety and Health (NIOSH). The findings and conclusions in this report are those of the authors and do not necessarily represent the views of the National Institute for Occupational Safety and Health.
ConclusionNo association was observed between the wave components of the BAEP and the estimated blood lead levels of 12.2μg/dL (±5.7μg/dL) in children exposed to lead. BAEP does not seem to be the most sensitive method to evaluate children with low blood lead levels.
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Alvarenga KF, Morata TC, Lopes AC, Feniman MR, Corteletti LC. Brainstem auditory evoked potentials in children with lead exposure. Braz J Otorhinolaryngol. 2015;81:37–43.


