
Facial plastic and reconstructive surgery involves the use of surgical procedures to achieve esthetic and functional improvement. It can be used for traumatic, congenital, or developmental injuries. Medicine, with an emphasis on facial plastic surgery, has made progress in several areas, including rhinoplasty, providing good long-term results and higher patient satisfaction.
ObjectiveTo evaluate cases of rhinoplasty and its subtypes in a referral center, and to understand the relevance of teaching rhinoplasty techniques in a service of otolaryngology residency.
MethodsA retrospective study that assessed 325 rhinoplasties performed by third-year medical residents under the supervision of chief residents in charge of the Service of Facial Plastic Surgery in this hospital was conducted from January of 2003 to August of 2012. The Service Protocol included the following subtypes: functional, esthetic, post-traumatic, revision, and reconstructive rhinoseptoplasty.
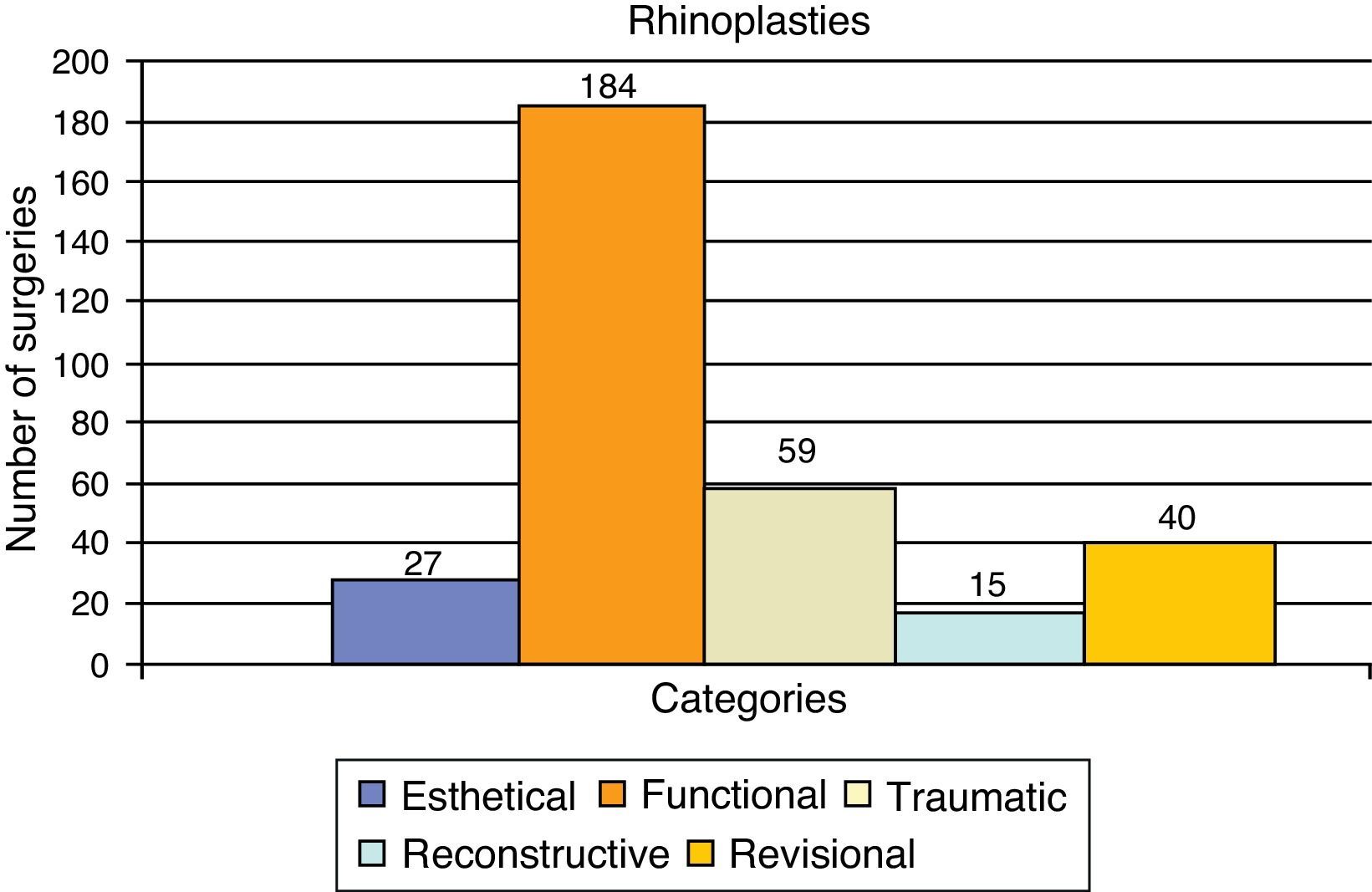
ResultsOf the rhinoplasties performed 184 (56.21%) were functional, 59 (18.15%) were post-traumatic, 27 were (8.30%) esthetic, 15 were (4.61%) reconstructive, and 40 (12.30%) were revision procedures.
ConclusionFunctional rhinoseptoplasties were the most prevalent type, which highlights the relevance of teaching surgical techniques, not only for septoplasty, but also the inclusion of rhinoplasty techniques in teaching centers.
A cirurgia estética e reconstrutora têm por objetivo a utilização de procedimentos cirúrgicos para alcançar melhora estética e funcional. Pode ser utilizada para lesões traumáticas, congênitas ou de desenvolvimento. A Medicina, com ênfase na plástica facial, obteve avanços nas mais diversas áreas, inclusive na rinoplastia, permitindo bons resultados a longo prazo e maior satisfação dos pacientes.
ObjetivoAvaliar a casuística do setor de rinoplastia e suas subdivisões em um centro de referência. Compreender a relevância do ensino das técnicas de rinoplastia em um serviço de residência médica de otorrinolaringologia.
MétodoEstudo retrospectivo onde foram analisados 325 rinoplastias, realizadas por médicos residentes do terceiro ano com supervisão dos preceptores responsáveis pelo serviço de Cirurgia Plástica da Face desse hospital, no período de janeiro de 2003 a agosto de 2012. O protocolo do serviço foi preenchido com enfoque nas seguintes subdivisões: rinosseptoplastia funcional, estética, pós-traumática, revisional e reconstrutora.
ResultadosDas rinoplastias realizadas, 184 (56,21%) foram funcionais, 59 (18,15%) pós-traumáticas, 27 (8,30%) estéticas, 15 (4,61%) reconstrutoras e 40 (12,30%) revisionais.
ConclusãoAs rinosseptoplastias funcionais foram as mais prevalentes, o que mostra a importância do ensino, não somente das técnicas de septoplastias, mas também, da inclusão do aprendizado de técnicas de rinoplastias em centros de ensino.
Cosmetic surgeries are on the rise, and among them, rhinoplasty is one of the most commonly performed. Through the use of a good technical basis in basic rhinoseptoplasty surgery, it is possible to treat approximately 95% of primary patients seen in a private practice of esthetic surgery, demonstrating the increasing need for inclusion of more refined techniques of rhinoplasty in routine otorhinolaryngology.1
In the late 19th century, rhinoplasty was nearly exclusively reconstructive surgery for large nasal mutilations.2 In the early 20th century, it was rapidly disseminated worldwide as an esthetic procedure, but in the 21st century, it has become more conservative, with modeling techniques rather than cartilage resection and with a significant reduction in aggressive osteotomies.3,4
The number of rhinoplasties and their subtypes (functional, esthetic, reconstructive, revision, and post-traumatic surgeries) has significantly increased since the mid-20th century.3,5 However, the nose represents a complex anatomical region, in which small functional alterations can cause great harm to the patient.6 Thus, the study of rhinoplasty techniques associated with those of septoplasty has gained prominence in referral otolaryngology services, which are regarded as professional generation centers, with the greatest responsibility for the training of these professionals.2,4
The present study aimed to evaluate a series of patients who underwent rhinoplasty in a referral center, focusing on the esthetic, functional, post-traumatic, reconstructive, and revision subtypes. Reconstructive surgeries are those performed to correct defects due to loss of substance (e.g., after tumor resection); revision procedures are surgical re-interventions, either performed by the same surgeon or another one; post-traumatic surgeries are those performed due to injuries resulting from external causes; functional procedures consist of any approach aiming at respiratory function correction; and esthetic procedures are purely cosmetic surgeries.
MethodsThis was a cross-sectional, historical cohort study performed through the collection of data from medical records and service protocols, from January 2003 to August 2012.7 The inclusion criteria were all patients submitted to rhinoplasty during that period, with records containing all clinical and surgical information, while the exclusion criteria were patients whose records were incomplete. There were no clinical conditions of exclusion.
Patients underwent general clinical and otorhinolaryngological assessment, preoperative evaluation, in addition to photo sessions and surgical procedure scheduling by profilometry. The following parameters were evaluated: facial thirds, facial fifths, nasofrontal and nasolabial angles, columella-lobule angle, natural horizontal facial plane, nasal length, and tip projection.8
Third-year residents performed the rhinoplasty surgeries, under the supervision of the chief residents in charge of the Service of Facial Plastic Surgery of the Otolaryngology Department of this hospital. Whenever necessary, the chief residents intervened in the surgery, correcting faults, developing the technique, and finalizing the surgery within a safe time period for the patient. All procedures were performed under local or general anesthesia, and most often, the patient was discharged within 24h.
Postoperatively, patients underwent ambulatory monitoring, returning for consultations seven, 15, and 30 days after the surgery, with follow-up visits at three months, six months, and annually thereafter. On these occasions, new photographs were taken and surgical results were analyzed.
The protocol, modified from the literature to adapt to this service,9 was completed for the following subtypes of rhinoplasty: functional rhinoseptoplasty, cosmetic, reconstructive, revision, and post-traumatic rhinoplasty. All patients signed an informed consent. Data regarding the type of surgery performed were carefully verified from the patients’ surgical records and processed in Microsoft Excel®.
The study was approved by the Ethics Committee on Human Research of the Hospital, under number 0138.0.203.000-11.
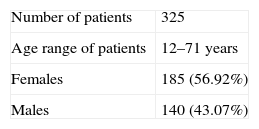
ResultsAfter applying the inclusion and exclusion criteria, a total of 325 patients were identified. Of these, 185 (56.92%) were females and 140 (43.07%) were males. The mean age was 30.9±7.5 years (Table 1).
Of the 325 selected rhinoplasties, 184 (56.61%) were functional, 59 (18.15%) post-traumatic, 27 (8.30%) esthetic, 15 (4.61%) reconstructive, and 40 (12.30%) were revision surgeries (Fig. 1).

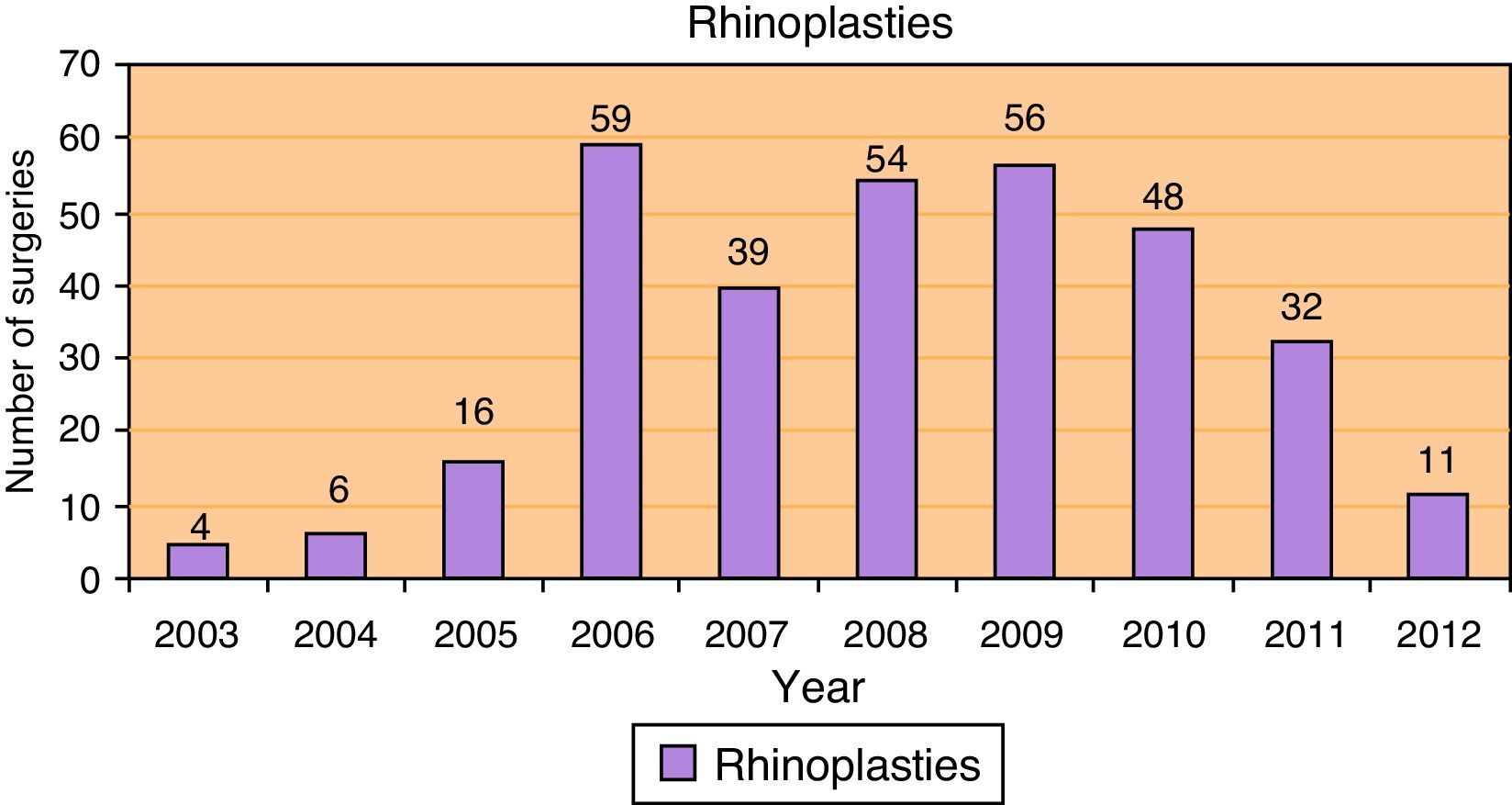
The mean number of surgeries performed per year was 32.5, with a minimum of four surgeries in 2003 and a maximum of 59 surgeries in 2006 (Fig. 2).
Discussion
The popularity of facial plastic surgeries has grown from the mid-20th century and shows a strong tendency toward higher growth, mainly influenced by the expansion of the beauty and body metamorphosis industries. Brazil is currently the second largest market in number of facial plastic surgeries, second only to the United States.2,10
Of all the facial cosmetic procedures, face-lifts, facial liposuction, blepharoplasty, and rhinoplasty are predominant. Rhinoplasty, however, is the most frequently performed facial esthetic surgery in the United States, mainly due to its strong esthetical and functional characteristics.9,10
Reparative rhinoplasty for the reconstruction of large nasal mutilations has become more conservative, with greater use of modeling maneuvers and with less cartilage resection and a significant reduction of the need for aggressive osteotomies. Moreover, its association with more refined techniques of septoplasty has resulted in greatly improved functional outcomes.4,11 However, even today, these procedures require extensive technical and scientific knowledge, placing great responsibility on the referral centers that have the obligation to provide the education, training, and experience in this area.9
In the present study (Fig. 1), we observed a high prevalence of functional surgeries (184; 56.61%), which highlights the increasing need for improved rhinoseptoplasty techniques, rather than exclusively septoplasty techniques. Tanna et al.2 reported medical residency as the main factor in the learning curve in this type of procedure, and cited an average of 15 surgeries/year/resident in major referral centers in the United States. This is in line with our study, which shows an average of 32.5 surgeries/year for two third-year medical residents, providing a major contribution to professional training in facial plastic surgery.
ConclusionRhinoplasty requires surgical skills and experience to achieve good results. The authors believe that residents should perform such surgeries, and training centers can provide a sufficient number and frequency of cases. There is a clear prevalence of respiratory symptoms in patients seeking otorhinolaryngological evaluation for this procedure. Therefore, given the high overall prevalence of functional rhinoseptoplasties, the importance of teaching rhinoplasty techniques, associated with septoplasty and other techniques aimed at improvement of nasal airflow, is noteworthy.
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Nunes FB, Crosara PF, Oliveira IS, Evangelista LF, Rodrigues DS, Becker HM, et al. Classification of rhinoplasties performed in an otorhinolaryngology referral center in Brazil. Braz J Otorhinolaryngol. 2014;80:476–9.
Institution: Department of Otorhinolaryngology, Hospital das Clínicas (HC), Universidade Federal de Minas Gerais (UFMG), Belo Horizonte, MG, Brazil.
gology is pleased to honor the reviewers


