
Extranodal NK/T-Cell lymphoma, nasal type (NKTLN) is a disease that mainly affects the nasal cavity and the paranasal sinuses. Early nasal symptoms are nonspecific, simulating sinus infection. With disease progression, necrosis of the nasal mucosa increases, hindering histological diagnosis. Thus, multiple biopsies may be necessary until definitive diagnosis. Most studies on NKTLN address the hematological and immunological aspects of the disease.
ObjectivesTo present data from a Brazilian quaternary hospital, with emphasis on the clinical aspects of the disease, and to correlate the findings with the most recent literature data.
MethodsCase study of seven patient files.
ResultsPatients were evaluated on their medical history, number of biopsies necessary, association with Epstein–Barr virus, treatment, and outcome. All patients had nonspecific nasal complaints and underwent at least three cycles of antibiotic therapy. The earlier a biopsy was performed, the fewer biopsies were required to diagnose the disease and start treatment. However, this fact did not translate into better prognosis.
ConclusionThe otolaryngologist plays a fundamental role in the prognosis of NKTLN and can shorten time between symptom onset and treatment of the patient.
O linfoma extranodal de células NK/T tipo nasal (LNKTN) é uma doença que acomete preferencialmente a cavidade nasal e os seios paranasais. Os sintomas nasais iniciais são inespecíficos, mimetizando um quadro de infecção nasossinusal. Com a progressão da doença, aumenta a necrose da mucosa nasossinusal, dificultando o diagnóstico histológico e podendo ser necessárias múltiplas biópsias até o diagnóstico definitivo. A maioria dos estudos sobre o LNKTN aborda aspectos imunológicos e hematológicos da doença.
ObjetivoApresentar a casuística de um hospital quaternário brasileiro, destacando os aspectos clínicos dos pacientes e correlacionando aos achados mais recentes da literatura.
MétodoEstudo de casos de sete pacientes.
ResultadosPacientes foram avaliados quanto a aspectos de sua história clínica, número de biópsias necessárias, associação ao EBV, tratamento e evolução. Todos iniciaram o quadro com queixas inespecíficas nasais e foram submetidos a pelo menos três ciclos de antibióticos. Quanto mais precocemente a biópsia foi realizada, menos biópsias foram necessárias para se obter o diagnóstico e iniciar o tratamento. Entretanto, esta situação não refletiu num melhor prognóstico dos pacientes.
ConclusãoO otorrinolaringologista tem papel fundamental no prognóstico do LNKTN, podendo encurtar o tempo entre o início dos sintomas e o tratamento do paciente.
Extranodal NK/T-Cell lymphoma, nasal type (NKTLN) is a disease that mainly affects the nasal cavity and paranasal sinuses,1 and thus, the otorhinolaryngologist is invariably the first specialist to evaluate these patients. It is a rare disease, more frequent in middle-aged adult males, with high prevalence in East Asia, where it represents 3–10% of all malignant tumors, and is the most prevalent lymphoma in Amerindian descendants from South and Central America.1–3 Another factor that plays an important role in the pathogenesis of the disease is infection by the Epstein–Barr virus (EBV).4,5
Historically, NKTLN has had different names. Due to the difficulty in clearly determining the physiopathological mechanism of the disease in the past, the terms “Lethal Midline Granuloma” and “Midfacial Granuloma” included, in addition to NKTLN, other diseases with aggressive evolution that also affected the middle portion of the face, such as Wegener's granulomatosis and infectious diseases such as Leishmaniasis. The terms “polymorphic reticulosis” and “angiocentric lymphoma” were attempts to histopathologically characterize NKTLN, but were also discarded, as these patterns are not always present.1,6,7 The current name was adopted by the Revised European-American Lymphoma Classification (REAL), proposed by the WHO in 2001 and reinforced in 2008.8
In most cases, the initial nasal symptoms are unspecific, such as rhinorrhea, nasal obstruction, and epistaxis, mimicking a picture of sinonasal infection, which makes it difficult to establish the diagnosis of NKTLN.1 With disease progression, edema, necrosis, and destruction of adjacent structures occur, which can cause the collapse of the lateral wall of the nasal cavity and oronasal fistula.
In patients at an advanced stage of the disease, with abundant necrosis and little healthy tissue, there is difficulty in establishing the histological diagnosis and multiple biopsies may be required until a definitive diagnosis is achieved.1,9 Extra-nasal manifestations are also possible, which may be associated with nasal injury; the main affected sites are: skin, larynx, testes, gastrointestinal tract, and kidneys.1,10 Lymphadenopathy, either inflammatory or tumor-related, can also be observed, especially in patients with nasal involvement.10
Since most studies available in the literature on NKTLN assessed samples of Asian origin or have their primary focus on the hematological and immunological aspects, this study aimed to assess a sample from a Brazilian quaternary hospital, highlighting the clinical aspects of patients and correlating them to the most recent literature findings.
MethodThe present study is a series of cases based on medical records of patients treated at the Otorhinolaryngology Outpatient Clinic of this institution between January 2005 and June 2013.
The study included all patients diagnosed with NKTLN, selected through the electronic database of the Pathology Department of this institution.
The study was approved by the Research Ethics Committee, opinion No. 444,035 of October 18, 2013.
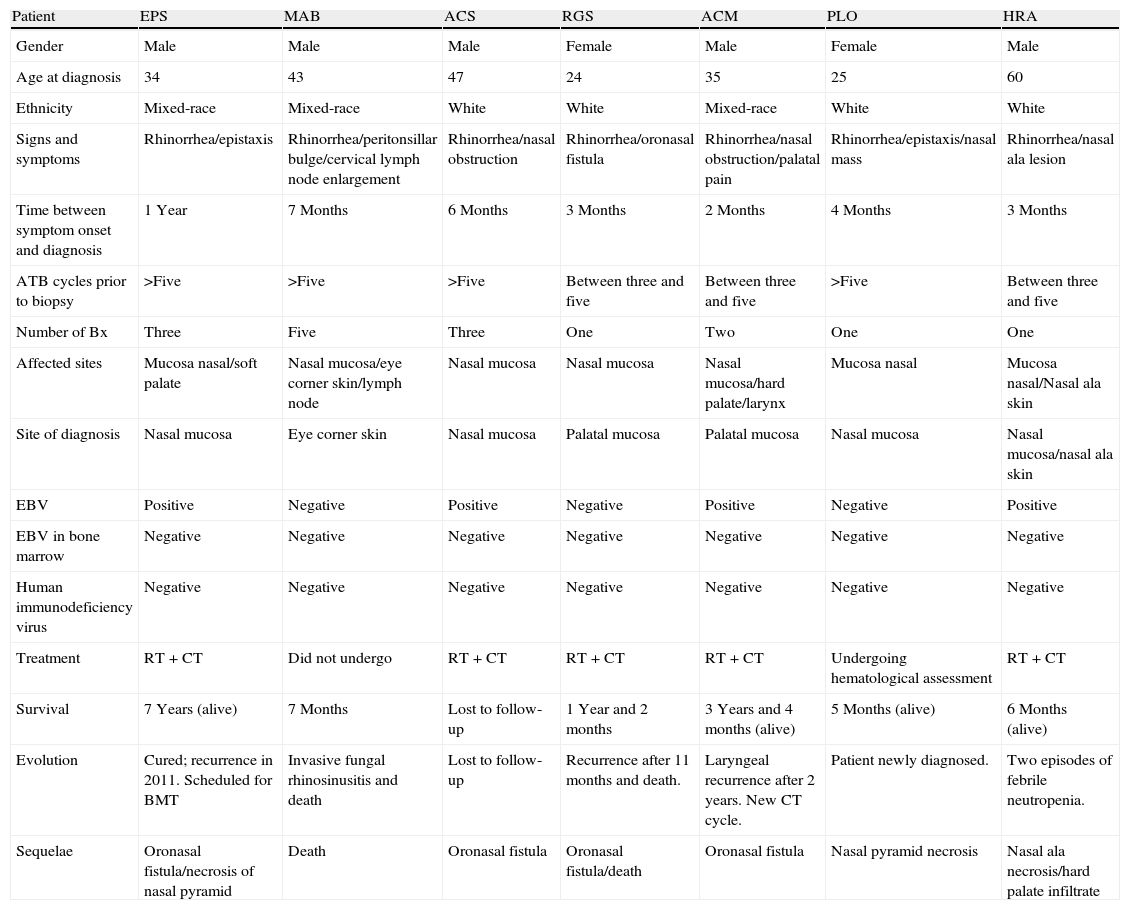
ResultsThe results of the study were shown in Table 1.
Results of the study.
| Patient | EPS | MAB | ACS | RGS | ACM | PLO | HRA |
| Gender | Male | Male | Male | Female | Male | Female | Male |
| Age at diagnosis | 34 | 43 | 47 | 24 | 35 | 25 | 60 |
| Ethnicity | Mixed-race | Mixed-race | White | White | Mixed-race | White | White |
| Signs and symptoms | Rhinorrhea/epistaxis | Rhinorrhea/peritonsillar bulge/cervical lymph node enlargement | Rhinorrhea/nasal obstruction | Rhinorrhea/oronasal fistula | Rhinorrhea/nasal obstruction/palatal pain | Rhinorrhea/epistaxis/nasal mass | Rhinorrhea/nasal ala lesion |
| Time between symptom onset and diagnosis | 1 Year | 7 Months | 6 Months | 3 Months | 2 Months | 4 Months | 3 Months |
| ATB cycles prior to biopsy | >Five | >Five | >Five | Between three and five | Between three and five | >Five | Between three and five |
| Number of Bx | Three | Five | Three | One | Two | One | One |
| Affected sites | Mucosa nasal/soft palate | Nasal mucosa/eye corner skin/lymph node | Nasal mucosa | Nasal mucosa | Nasal mucosa/hard palate/larynx | Mucosa nasal | Mucosa nasal/Nasal ala skin |
| Site of diagnosis | Nasal mucosa | Eye corner skin | Nasal mucosa | Palatal mucosa | Palatal mucosa | Nasal mucosa | Nasal mucosa/nasal ala skin |
| EBV | Positive | Negative | Positive | Negative | Positive | Negative | Positive |
| EBV in bone marrow | Negative | Negative | Negative | Negative | Negative | Negative | Negative |
| Human immunodeficiency virus | Negative | Negative | Negative | Negative | Negative | Negative | Negative |
| Treatment | RT+CT | Did not undergo | RT+CT | RT+CT | RT+CT | Undergoing hematological assessment | RT+CT |
| Survival | 7 Years (alive) | 7 Months | Lost to follow-up | 1 Year and 2 months | 3 Years and 4 months (alive) | 5 Months (alive) | 6 Months (alive) |
| Evolution | Cured; recurrence in 2011. Scheduled for BMT | Invasive fungal rhinosinusitis and death | Lost to follow-up | Recurrence after 11 months and death. | Laryngeal recurrence after 2 years. New CT cycle. | Patient newly diagnosed. | Two episodes of febrile neutropenia. |
| Sequelae | Oronasal fistula/necrosis of nasal pyramid | Death | Oronasal fistula | Oronasal fistula/death | Oronasal fistula | Nasal pyramid necrosis | Nasal ala necrosis/hard palate infiltrate |
EBV, Epstein–Barr virus; RT, radiotherapy; CT, chemotherapy; BMT, bone marrow transplantation.
The differences and similarities in presentation, diagnosis, treatment and outcome of documented clinical cases represent a diversified overview of clinical-otorhinolaryngological aspects of NKTLN.
Of the seven patients (Table 1), five were adult males and four were between 34 and 47 years, resembling the patient profile more often observed in the literature.1,2 However, none had Asian or Amerindian ancestry.
The initial clinical picture included at least one sinonasal symptom in all cases (rhinorrhea/nasal obstruction) and patients were treated with antibiotics for the treatment of acute rhinosinusitis. This situation delays the diagnosis and treatment of patients with NKTLN who, in general, only undergo biopsy after several antibiotic treatments. In the present series, the time between symptom onset and the histopathological diagnosis of NKTLN ranged between 2 months and 1 year.
As the indication for the biopsy is postponed, the evolution of NKTLN shows an increase in the amount of edema, crusting, bone erosion, and necrosis in the sinonasal mucosa, impairing the histopathological diagnosis in the presence of little significant samples of disease-affected tissue.1 Thus, the earlier the biopsy is performed, the greater the chance of obtaining a representative disease sample, reducing the number of required biopsies9 The diagnoses within 3 months of the onset of symptoms in patients RGS, ACM, and HRA was attained with one or two biopsies. In the patients, who had symptoms for 6 months or more, three or more biopsies were necessary.
Sometimes, due to the prevalence of necrotic tissues, and secondary infection in the nasal cavity, depending on the manner in which the lymphoma spreads, the NKTLN diagnosis may be achieved by a biopsy of other disease sites, such as the palate and skin, which we noted in patients MAB, RGS, and ACM. Dissemination to other organs is atypical and may involve the lungs, gastrointestinal tract, kidneys, pancreas, testes, and brain, in addition to the skin.1,2 Even rarer is a primary initial presentation of NKTLN outside the midfacial region; when this occurs, it usually involves the skin.1,2
Another problem caused by the presence of necrosis and crusting of the nasal mucosa is the predisposition to secondary infections, especially by fungi. This condition can be a confounding factor in the interpretation of the histopathological examination, leading to a misdiagnosis of isolated fungal infection in a patient who actually has NKTLN with secondary fungal infection. Additionally, secondary infection can significantly worsen the prognosis of patients with NKTLN by worsening the patient's clinical condition, and because it is a condition that contraindicates chemotherapy administration.1
Patient MAB underwent biopsies on four different occasions, in different sites, always with presence of Mucor and necrosis in the histopathological diagnosis. As the antifungal treatment had shown only partial improvement and a new lesion had appeared at the corner of the eye, this site was chosen for the fifth biopsy, which diagnosed NKTLN. However, as the patient was already weakened clinically, chemotherapy could not be initiated and the patient died during hospitalization.
The presence of EBV in tissue biopsy analysis was positive in four of the seven patients. The association between EBV and NKTLN has been well established in the literature, although its mechanism of action is still being studied.4,5,10 It is also believed that the EBV viral load may be a prognostic factor in the evolution of NKTLN.4,10 The presence of EBV was not detected in bone marrow and no patient was HIV positive.
Currently, there is no standardized treatment protocol for NKTLN, and the combination of radiotherapy and chemotherapy is routinely used.1 All our patients were treated in this manner, except MAB, who died before treatment, and PLO, who had been newly diagnosed. Another therapeutic possibility currently being investigated is bone marrow transplantation; patient EPS has been scheduled to undergo this procedure.
The most common sequelae observed in the patients were oronasal fistulas, present in four patients. A fifth patient (HRA) had an infiltrative lesion in the hard palate, with probable progression to fistula. Of the other two remaining patients, one was newly diagnosed (PLO) and the other showed rapid disease progression, leading to death (MAB). Another frequently observed sequela was nasal pyramid involvement, observed in three patients. Two patients had complications: MAB had invasive fungal rhinosinusitis even before the diagnosis of NKTLN, and HRA had two episodes of febrile neutropenia. Two patients had extra-nasal involvement: ACM, laryngeal; and MAB, eye corner skin and cervical lymph node. In the literature, the extra-nasal manifestation of NKTLN is seen in one in every three to four patients.10
As for disease evolution and behavior, the patients studied had varied characteristics. MAB had an evolution of only 7 months between symptom onset and death, whereas EPS remains alive 7 years after symptom onset, in spite of a late-onset diagnosis (only after 1 year of symptom onset) and after tumor recurrence in the nasal cavity. In addition to EPS, two other patients also had recurrence: RGS had tumor recurrence in the nasal cavity and died; and ACM had tumor recurrence in the larynx and underwent a new chemotherapy cycle. In general, NKTLN has a poor outcome, with overall 5-year survival ranging from 20 to 65%.10–12
ConclusionAlthough rare, the diagnosis of NKTLN should always be considered in cases of repeated rhinosinusitis refractory to medical treatment. The otolaryngologist plays a fundamental role in the prognosis of this disease, and may shorten the time between symptom onset and start of treatment through an appropriate clinical history that precedes biopsies. Furthermore, it is also important to perform the removal of necrotic tissue in the nasal cavity, preventing opportunistic infections and allowing the patient to be submitted to radiation therapy and chemotherapy in good clinical condition.
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Miyake MM, Oliveira MV, Miyake MM, Garcia JO, Granato L. Clinical and otorhinolaryngological aspects of extranodal NK/T cell lymphoma, nasal type. Braz J Otorhinolaryngol. 2014;80:325–9.
Institution: Department of Otorhinolaryngology of Santa Casa de Misericórdia de São Paulo, São Paulo, SP, Brazil.
gology is pleased to honor the reviewers


