
For many years, excessive caffeine consumption has been touted as an aggravating factor for tinnitus. The pathophysiology behind this effect is probably related to the blockage of adenosine receptors by the action of caffeine on the central nervous system.
ObjectiveTo evaluate the effects of reduction of coffee consumption on tinnitus sensation and to identify subgroups more prone to benefit from this therapeutic strategy.
Study designProspective.
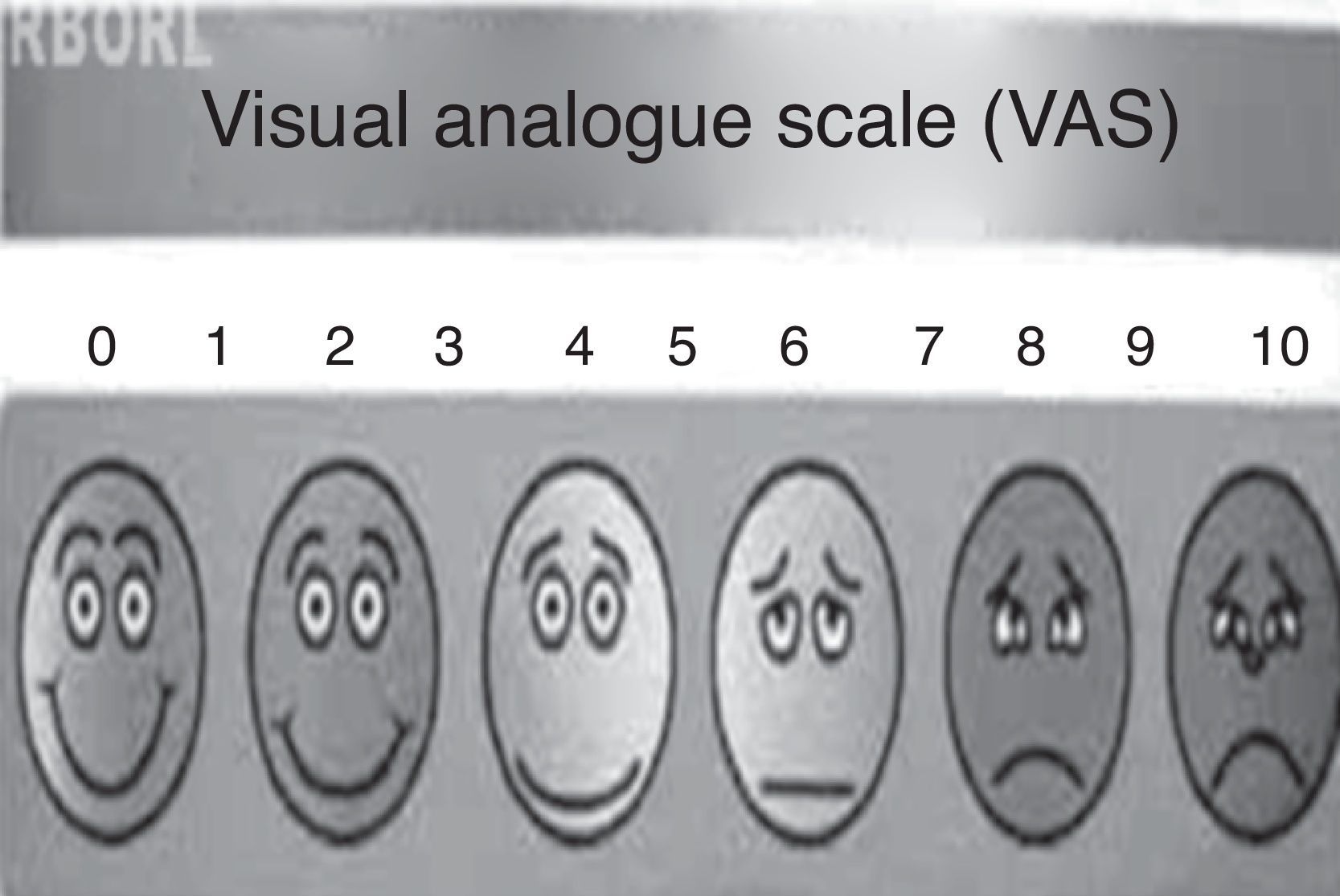
MethodsTwenty-six tinnitus patients who consumed at least 150mL of coffee per day were selected. All were asked to reduce their coffee consumption. The Tinnitus Handicap Inventory (THI) questionnaire was completed by the patients before and after the reduction of coffee consumption, as well as a visual-analog scale (VAS) graduated from 1 to 10.
ResultsTHI and VAS scores were significantly reduced (p<0.05). In the subgroups less than 60 years old, bilateral tinnitus and daily coffee consumption between 150 and 300mL showed a significantly greater reduction of THI and VAS scores.
ConclusionPatients under 60 years of age with bilateral tinnitus and daily coffee consumption between 150 and 300mL are more prone to benefit from consumption reduction. Thirty-day observation periods may be helpful for a better therapeutical decision.
O consumo abusivo de cafeína vem sendo descrito como fator de piora e causa do zumbido há muitos anos. A fisiopatologia deste efeito está provavelmente relacionada ao bloqueio dos receptores inibitórios adenosínicos pela cafeína no sistema nervoso central.
ObjetivoAvaliar os efeitos da redução do consumo de cafeína na percepção do zumbido e identificar subgrupos de pacientes mais propensos a benefícios com esta proposta.
Tipo de estudoProspectivo.
MétodosSelecionados 26 pacientes com zumbido neurossensorial e consumo diário superior a 150mL de café. Os efeitos da redução do consumo foram avaliados através do Tinnitus Handicap Inventory (THI) e da escala visual-análoga (EVA).
ResultadosHouve redução estatisticamente significativa (p<0.05) nos escores do THI e EVA. Nos subgrupos com idade inferior a 60 anos, zumbido bilateral e consumo diário de café entre 150 e 300mL apresentaram maior redução dos escores THI e EVA.
ConclusãoEm pacientes com idade inferior a 60 anos, zumbido bilateral e consumo diário de café entre 150 e 300mL apresentaram benefícios com a redução no consumo diário de cafeína. Períodos observacionais de 30 dias podem ser úteis para a decisão terapêutica.
Caffeine, also known as methyltheobromin, is part of the group of methylxanthines, and is considered the most widely used psychoactive substance in the world. The majority of its consumption is derived from dietary sources such as coffee, tea, cola soft drinks, and chocolate; the most striking behavioral effects are increases in alertness, energy, and concentration skills. These effects are more pronounced after ingestion of small to moderate amounts (50–300mg).1
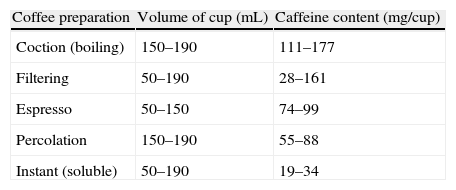
The caffeine content by coffee cup varies depends on the form of preparation (Table 1).1 In Brazil, the per capita consumption, according to the Associação Brasileira de Indústrias do Café (ABIC), is currently about 73L per year, and the filtration method of preparation is the most commonly used.2 A worldwide trend toward increased coffee consumption has been noted. The caffeine content of other beverages varies, on average, from 32 to 42mg/150mL (tea), 32 to 70mg/330mL (cola beverages), and approximately 4mg/150mL (chocolate flavored milk).1
Amount of caffeine in various forms of coffee preparation.
| Coffee preparation | Volume of cup (mL) | Caffeine content (mg/cup) |
| Coction (boiling) | 150–190 | 111–177 |
| Filtering | 50–190 | 28–161 |
| Espresso | 50–150 | 74–99 |
| Percolation | 150–190 | 55–88 |
| Instant (soluble) | 50–190 | 19–34 |
The absorption of caffeine in the gastrointestinal tract is rapid, reaching 99% after 45min. Peak plasma levels are achieved between 15 and 120min after oral ingestion, and the half-life is about 2.5–4.5h. Caffeine is metabolized by the liver.1
Currently, most authors believe that the main mechanism of action of caffeine is the antagonism of adenosinic receptors.1,3–5 Adenosine reduces the firing rate of neurons, exerting an inhibitory effect on synaptic transmission and in the release of various neurotransmitters. In 1993, Daly observed increased brain levels of norepinephrine, glutamate, and adrenaline after caffeine intake.3 The adenosinic receptors involved with the effects of caffeine are A1 and A2. Neurostimulant effects of caffeine have been demonstrated in functional imaging studies.6
A2 adenosinic receptors interact with dopaminergic receptors in the nucleus striatum and nucleus accumbens by modulating them. Therefore, the blockage of these receptors, exerted by caffeine, could potentiate the dopaminergic neurotransmission.1
Other demonstrated actions of caffeine include increased release of intracellular calcium and inhibition of phosphodiesterases; seemingly, these mechanisms are unrelated to the central effects of caffeine.1
In addition to the neuroexcitatory effects, caffeine also has a vasoconstrictor effect, and this is the predominant effect at higher doses.6 Studies with blood oxygenation level-dependant (BOLD) functional magnetic resonance imaging demonstrated a reduction in cerebral perfusion after caffeine intake. Some authors believe that the neurostimulant effects of caffeine are due primarily to its action on A1 receptors, whereas the vasoconstrictor effects are related to its effects on A2 receptors.6
Based on these neurostimulant effects of caffeine, several studies addressed the effects of this substance on the central auditory pathways.4–8 Lorist et al. found improvement of the central auditory processing after caffeine intake5 and Kawamura et al.6 found increase in the amplitude and area of P300 approximately 30min after caffeine ingestion.
Dixit et al.4, also studying the effects of caffeine on P300, observed an increase in P3 amplitude and reduced reaction time, indicating facilitation of auditory processing and acceleration of motor responses. In another study, the same authors found a significant reduction in latencies of waves IV and V in auditory brainstem potentials (ABR), and a significant decrease in the I–V interval.9
In the cochlea, it was demonstrated that caffeine induced shortening of outer hair cells (OHC).10–12 This fact would have some bearing on the rapid contraction of OHC, increasing the excitability of the peripheral auditory pathwaysThere is disagreement about the events involved in this shortening. Slepecky et al.10, in a 1988 study, suggested that the shortening of OHC occurs by mechanisms associated with rianodinic receptors. Conversely, Yamamoto et al.11, in 1995, suggested that OHC depolarization occurs by potassium channel blockage. Finally, Skellett et al.12, in a study from 1995, suggested an osmotic mechanism.
Most clinical studies on the effects of caffeine in otoneurology refer to changes in the vestibular system.13–15 Several authors suggest a daily intake of up to three small cups (50mL) of filtered coffee as a beneficial practice for the treatment, and may even potentiate the therapeutic effects of some medications.15 Above this dose, the vasoconstrictor effects would predominate.
With regard to tinnitus, several authors suggest reducing the intake of caffeine as a supplementary treatment,16,17 but in the only controlled study ever conducted,18 beneficial effects of caffeine reduction on tinnitus were not observed. The main objective of this study was to assess whether sensorineural tinnitus patients can obtain some benefit from the reduction of caffeine intake. The secondary objective was to try to identify the subgroups of patients most likely to benefit with this strategy.
MethodsThis was a contemporary longitudinal cohort study. The sample size was initially determined considering as significant a difference of 20 points in THI score and of 2 points in VAS score (Fig. 1) in the interval from the beginning to the end of the study. Considering a statistical power of 0.80, the minimum sample size was set at 16 patients (for differences in THI scores and VSA inferior to 20 and 2 points, respectively, the required sample size would be even smaller).
.")
This study included 26 patients with sensorineural hearing loss, aged 24–76 years old, 15 males, treated in centers participating in the study between January 2008 and December 2009.
The following criteria were used:
Inclusion criteria
- •
Patients with tinnitus for more than six months
- •
Non-use of centrally acting drugs in the last six months
- •
Tympanogram type A-n
- •
Daily coffee intake exceeding three small cups/day (corresponding to 150mL/day)
- •
Age over 18 years old.
Exclusion criteria:
- •
THI<16 points
- •
Tinnitus of muscular and vascular origin
- •
Audiograms with conductive and mixed hearing loss
- •
Association with disorders of the temporomandibular joint.
At first visit, patients underwent a complete otorhinolaryngological exam. In the same consultation, tonal and vocal audiometry and imitanciometry were performed. Patients included in the study completed the Tinnitus Handicap Inventory (THI), in its version validated for Brazilian Portuguese,19 and also quantified the tinnitus with respect to the discomfort and intensity, according to a Visual Analog Scale (VAS) graded from 1 (minimal annoyance/intensity) to 10 (maximum annoyance/intensity).
After that, the patients were instructed to reduce their daily caffeine intake by at least 50% of their regular consumption; and all patients would consume quantities of less than 3 cups (50mL per cup). For instance, a patient who consumed an average of 600mL/day should reduce the intake to 150mL/day or less, and a patient who consumed 200mL/day should reduce this volume to 100mL/day or less.
A weekly contact by phone call was established to confirm the reduction of consumption. A new reassessment with THI and VAS was performed after 30 days, and all patients who did not achieve the aforementioned reduction goal were excluded.
The absolute change of the situation before/after the treatment was given by the following formula:
As the main criterion for reduction of THI, the level of seven points was used, i.e. a reduction of seven points in the score was considered as an improvement, according to the study by Zeman et al.20 Symptoms related to caffeine withdrawal were registered.
The statistical analysis consisted of the following tests:
Comparisons between the characteristics and improvement of THI were performed using Fisher's exact test (at least one expected frequency <5).
Then. the adjustment of the logistic model containing the characteristics with p-value <0.25 was performed. Only those characteristics with p-value <0.05 remained in the final model. All interactions were tested.
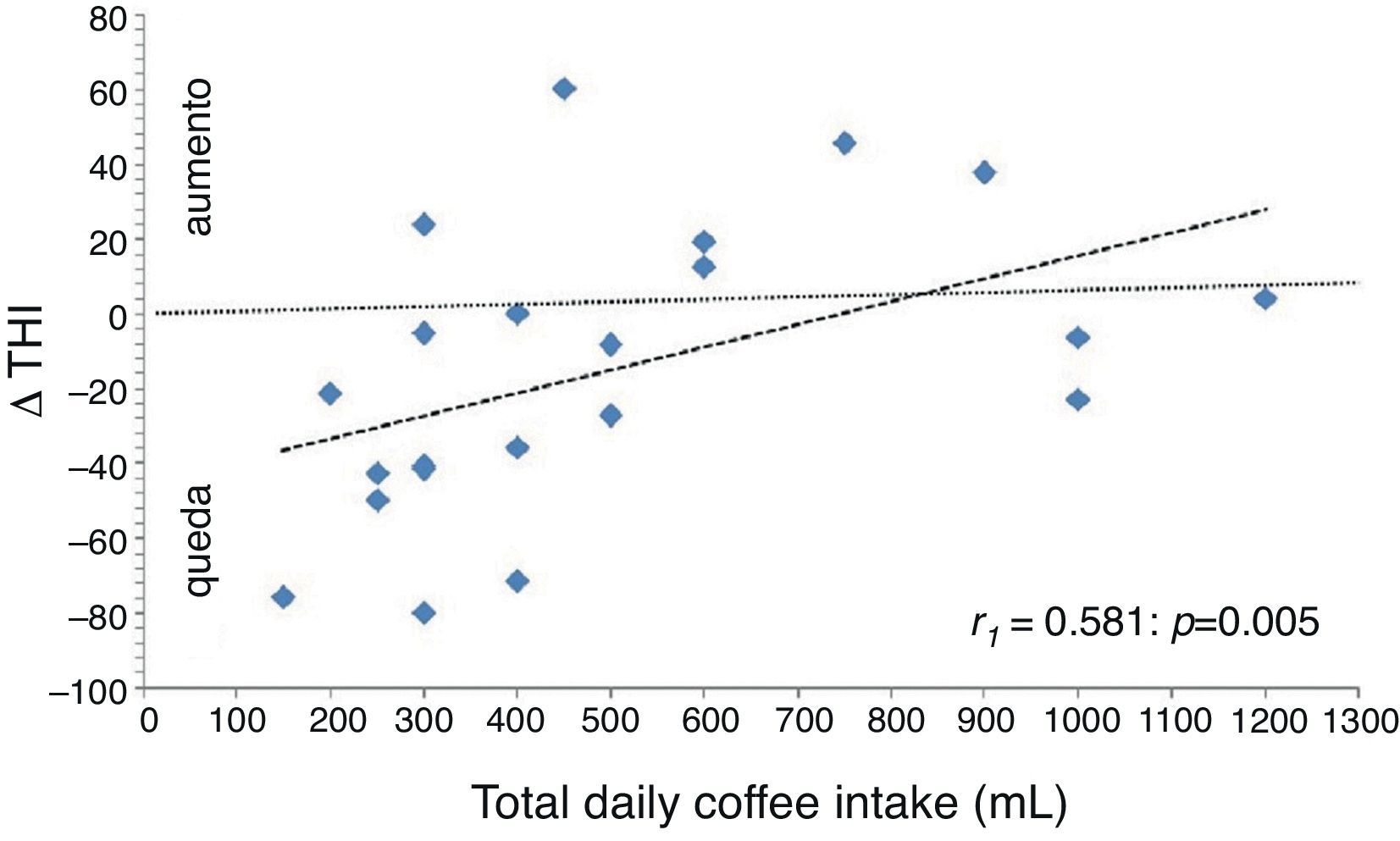
Finally, the Spearman correlation coefficient was applied to assess the degree of association between numerical variables and Δ THI/VAS.
The criterion for determining the significance was set at 5%. The statistical analysis was performed by SAS version 6.11 (SAS Institute, Inc. – Cary, North Carolina), R version 2.7.1, and EpiInfo version 6.04. The latter two are public domain programs.
The study was approved by the Ethics Committee for Medical Research under CAAE number – 0002.0.334.000-08.
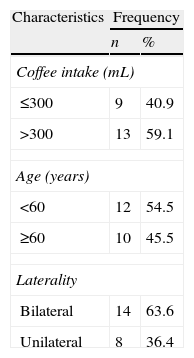
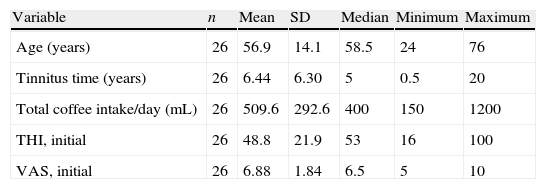
ResultsOf the 26 patients initially included, four did not return for the second evaluation. Table 2 shows general data of the sample, and Table 3 lists the subcategories distribution of the 22 patients who completed the study.
Description of coffee intake levels, age, and laterality of the sample.
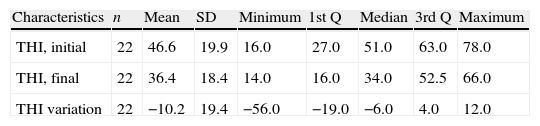
Of the 22 patients who completed the study, there was improvement in the THI scores (reduction of at least 7 points) in ten of them (45.5%). The observed mean decrease was 10.2 points for THI and 0.86 points for VSA; both were statistically significant (p=0.030 and 0.017, respectively). Table 4 presents the description of initial and final THI and the variation (final−initial).
Description of initial and final THI, and variation (Δ THI=final THI−initial THI).
| Characteristics | n | Mean | SD | Minimum | 1st Q | Median | 3rd Q | Maximum |
| THI, initial | 22 | 46.6 | 19.9 | 16.0 | 27.0 | 51.0 | 63.0 | 78.0 |
| THI, final | 22 | 36.4 | 18.4 | 14.0 | 16.0 | 34.0 | 52.5 | 66.0 |
| THI variation | 22 | −10.2 | 19.4 | −56.0 | −19.0 | −6.0 | 4.0 | 12.0 |
n, number of observations; SD, standard deviation; 1st Q, 1st quartile; 3rd Q, 3rd Quartile.
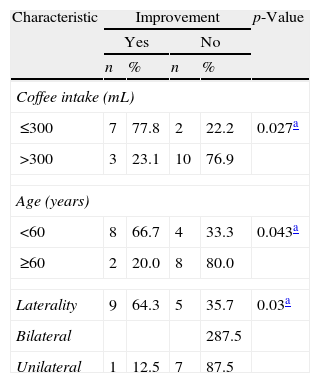
Table 5 shows the comparison of coffee intake, age, and laterality with improvement of THI. All features were selected for inclusion in the initial multivariate model.
Comparison between coffee intake, age and laterality and improvement of THI scores.
| Variable | n | Mean | SD | Median | Minimum | Maximum |
| Age (years) | 26 | 56.9 | 14.1 | 58.5 | 24 | 76 |
| Tinnitus time (years) | 26 | 6.44 | 6.30 | 5 | 0.5 | 20 |
| Total coffee intake/day (mL) | 26 | 509.6 | 292.6 | 400 | 150 | 1200 |
| THI, initial | 26 | 48.8 | 21.9 | 53 | 16 | 100 |
| VAS, initial | 26 | 6.88 | 1.84 | 6.5 | 5 | 10 |
SD, standard deviation.
Interpreting one of the intersections, for instance, among the nine patients who consumed up to 300mL of coffee per day, seven (77.8%) showed improvement in THI. Among the 13 patients who consumed more than 300mL/day, three (23.1%) showed improvement in THI. With a p-value of 0.027, this feature was selected to be included in the initial multivariate model.
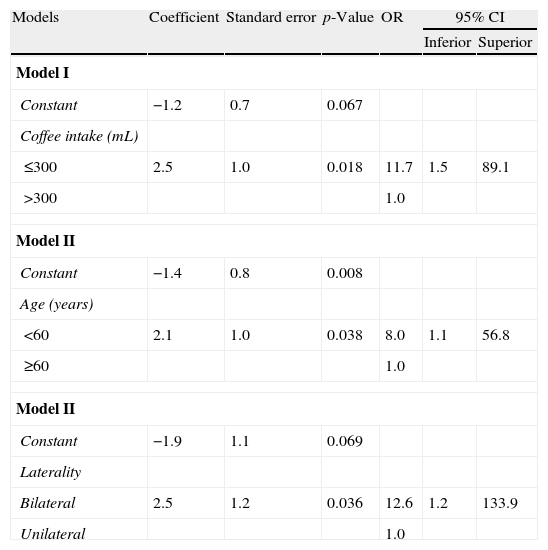
Table 6 shows the adjustments of the regression models. Three logistic regression models were elaborated.
Logistic regression model.
| Models | Coefficient | Standard error | p-Value | OR | 95% CI | |
| Inferior | Superior | |||||
| Model I | ||||||
| Constant | −1.2 | 0.7 | 0.067 | |||
| Coffee intake (mL) | ||||||
| ≤300 | 2.5 | 1.0 | 0.018 | 11.7 | 1.5 | 89.1 |
| >300 | 1.0 | |||||
| Model II | ||||||
| Constant | −1.4 | 0.8 | 0.008 | |||
| Age (years) | ||||||
| <60 | 2.1 | 1.0 | 0.038 | 8.0 | 1.1 | 56.8 |
| ≥60 | 1.0 | |||||
| Model II | ||||||
| Constant | −1.9 | 1.1 | 0.069 | |||
| Laterality | ||||||
| Bilateral | 2.5 | 1.2 | 0.036 | 12.6 | 1.2 | 133.9 |
| Unilateral | 1.0 | |||||
OR, odds ratio.
Thus, it was observed that those who consumed up to 300mL of coffee had approximately 12 times the chance of improvement in THI versus patients who consume more than 300mL of coffee (95% CI: 1.5–89.1).
In addition, patients younger than 60 years had eight times the chance of improvement in THI versus those aged over 60 years (95% CI 1.1–56.8). Patients with bilateral tinnitus had approximately 13 times the chance of improvement in THI versus those with unilateral tinnitus (95% CI, 1.2–133.9).
Analyzing the quantitative variable “coffee intake” (in mL) by the Spearman coefficient relative to Δ THI, Fig. 2 was obtained, confirming previous data (the higher the coffee intake, the lower the observed decrease in THI and VAS). Of the 22 patients who completed the study, only one (4.54%) showed a side effect (anxiety), possibly associated with the caffeine reduction. This patient consumed an average of 1200mL of coffee daily.
Discussion.")
Several articles on tinnitus have recommended the reduction of caffeine consumpion,16 but until recently, there were no specific studies on this subject. Theoretically, the stimulating action of caffeine on the central nervous system can play a role in the excitability of the auditory pathways and, therefore, can modify some clinical aspects of tinnitus.9
In a recent study (2010)18, the effects of the removal of caffeine on tinnitus in patients who consumed >150mg of caffeine daily were evaluated. In this pseudo-randomized, crossed-over, placebo controlled study of 66 patients, no evidence to justify a reduction in caffeine intake was found. Conversely, some side effects caused by withdrawal from caffeine were noted. According to the authors, these effects could also lead to a worsening of tinnitus.
However, this study failed to assess the possible effects of reducing the caffeine in different subgroups presenting such symptoms. Considering that the division of patients into different subgroups has been repeatedly used in the study on tinnitus treatment, the authors consider this issue of utmost importance.15,17 In addition, the analysis of the placebo effect in studies with caffeine can be extremely difficult, since chronic caffeine users can easily recognize the removal of this substance, regardless of the flavor of the beverage.1
Despite the statistical significance of data found in this study (a reduction of 10.2 points in THI and 0.86 points in VAS), it was observed that the effects of reducing caffeine intake on a tinnitus population as a whole would be small, according to the criteria used by Newman, which require as significant variations ≥20 points for THI.21 Only four (18.4%) of 22 patients showed such reduction. Conversely, the study by Zeman et al. demonstrated that differences of 6–7 points in THI scores are clinically relevant.20 In this case, ten patients (45.5% of the total sample) of this study fit into this profile. In the subgroup analysis, it was found that in subgroups with <60 years, bilateral tinnitus, and initial daily intake up to 300mL, the reduction in THI scores reaches close to 20 points. As a possible explanation for these differences, it may be surmised that elderly patients probably present a greater number of factors involved in the perception of tinnitus, such as presbycusis and use of multiple drugs to treat various medical conditions.
Patients with higher coffee intake may be more susceptible to symptoms after withdrawal from caffeine, as reported by St. Claire et al.18 Although only one of the present study's patients have shown signs compatible with withdrawal, the possibility that the worsening of the tinnitus is a symptom related to abstinence cannot be ruled out, which could outweigh any potential benefit of a reduction in caffeine intake.
Furthermore, the present study did not examine the percentage of caffeine reduction in each patient. Thus, considering the methodology used, the greater the amount of caffeine consumed, the greater the impact caused by the reduction of intake, which could be responsible for a possible worsening of tinnitus, related to caffeine withdrawal.
Considering the data, the authors believe that this represents an appropriate management strategy for each patient. While there are no data supporting the beneficial effects of reducing caffeine for all tinnitus patients, some subgroups, such as young patients with bilateral tinnitus and those with moderate caffeine intake are more likely to improve.
Much like the procedures for vestibular disturbances, and considering the possible effects of an abrupt reduction of caffeine intake, perhaps the best option is a gradual reduction, rather than the complete suppression of this substance. Periods of 30 days of observation appear to be sufficient to evaluate a possible beneficial effect and should be routinely used in therapeutic tests.
ConclusionThe results obtained in this study suggest that there is no justification for the universal restriction of caffeine intake as a treatment for all patients with tinnitus. However, patients younger than 60 years, with bilateral tinnitus, and with daily coffee intake between 150 and 300mL present greater benefits. The observation period of 30 days may be useful for the therapeutic decision.
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Figueiredo RR, Rates MJ, de Azevedo AA, Moreira RK, Penido NO. Effects of the reduction of caffeine consumption on tinnitus perception. Braz J Otorhinolaryngol. 2014;80:416–21.


