
Tinnitus is a multifactorial condition and its prevalence has increased on the past decades. The worldwide progressive increase of the use of cell phones has exposed the peripheral auditory pathways to a higher dose of electromagnetic radiofrequency radiation (EMRFR). Some tinnitus patients report that the abusive use of mobiles, especially when repeated in the same ear, might worsen ipsilateral tinnitus.
ObjectiveThe aim of this study was to evaluate the available evidence about the possible causal association between tinnitus and exposure to electromagnetic waves.
MethodsA literature review was performed searching for the following keywords: tinnitus, electromagnetic field, mobile phones, radio frequency, and electromagnetic hypersensitivity. We selected 165 articles that were considered clinically relevant in at least one of the subjects.
ResultsEMRFR can penetrate exposed tissues and safety exposure levels have been established. These waves provoke proved thermogenic effects and potential biological and genotoxic effects. Some individuals are more sensitive to electromagnetic exposure (electrosensitivity), and thus, present earlier symptoms. There may be a common pathophysiology between this electrosensitivity and tinnitus.
ConclusionThere are already reasonable evidences to suggest caution for using mobile phones to prevent auditory damage and the onset or worsening of tinnitus.
Zumbido é uma condição multifatorial cuja prevalência vem aumentando nas últimas décadas. Em todo o mundo, o aumento progressivo do uso de telefones celulares tem exposto as orelhas a uma maior carga de radiação eletromagnética de radiofrequência (REM-RF). Alguns pacientes com zumbido referem que o uso excessivo do telefone celular, especialmente quando sempre na mesma orelha, é um fator de piora do zumbido ipsilateral.
ObjetivoO objetivo deste trabalho foi avaliar as evidências disponíveis sobre a possível associação causal entre zumbido e exposição a ondas eletromagnéticas.
MétodoFoi realizada uma revisão de literatura com palavras-chave como: tinnitus, electromagnectic field, cellular phone, radiofrequency, electromagnectic hypersensitivity. Foram selecionados 165 artigos com maior relevância clínica em pelo menos um dos assuntos.
ResultadosAs REM-RF podem penetrar tecidos expostos e existem níveis seguros de exposição. Apresentam efeitos termogênicos comprovados e potenciais efeitos biológicos e genotóxicos. Alguns indivíduos são mais sensíveis à exposição eletromagnética (eletrossensibilidade) e, portanto, adquirem sintomas precocemente. A fisiopatologia da eletrossensibilidade pode ser semelhante à do zumbido.
ConclusãoConsideramos que há evidências suficientes que sugerem maior cautela para o uso desses aparelhos e assim prevenir lesões na via auditiva e o aparecimento/agravamento do zumbido.
Tinnitus is characterized by sound perception in the absence of an external source.1 Its prevalence has been increasing considerably in epidemiological studies, thus several international scientific events and publications have been devoted to explore this subject. Among adults from the United States, Shargorodsky2 found a prevalence of 25.3% for tinnitus, as opposed to 15% for the same population, published 15 years previously (National Institutes of Deafness and Other Communication Disorders, 1995).3 In a study with 506 children between 5 and 12 years old, 31% reported tinnitus according to rigorous criteria, and 19% were annoyed by the symptom.4
Although many people with tinnitus have no limitation on their quality of life, physicians, audiologists, and psychologists commonly receive patients who report that tinnitus leads to sleep disorders,5,6 lack of concentration, and impairment in social life and emotional balance.5,7
These findings justify the search for explanations for the gradual increase of tinnitus in different age groups. Plausible possibilities include increased longevity;8 early and enhanced exposure to loud noises (environmental or through earphones);8–10 higher levels of occupational stress, causing anxiety and depression;9,11,12 increased use of alcohol, tobacco, and illicit drugs; sedentary lifestyle; cardiovascular or metabolic diseases; etc.8
Another suspect being strongly considered for the increase of tinnitus onset is the exposure to electromagnetic radiation (EMR).13 In fact, in clinical practice, some patients have spontaneously mentioned hearing symptoms during or shortly after using cell phones, such as warmth or pressure in the ear that is in contact with the device, as well as tinnitus, reduced understanding, or distortion in hearing frequency. There is even a small group of patients who report tinnitus onset or worsening associated with living or working around cellular, radio, and TV antennas.
Non-ionizing electromagnetic radiofrequency radiation (EMRFR) is routinely used for telecommunications (radio, TV, WiFi, cellular and cordless phones, and radar). As exposure to this type of radiation is progressively increasing14 worldwide, there is a greater interest in its possible harmful effects on health.15 More sensitive individuals reported broad and unspecific symptoms like headache, dizziness, fatigue, memory impairment, sleep disorders, anxiety, myalgia, arthralgia, tearing, hearing loss, and tinnitus.16 The problematic issue regarding unspecific symptoms is that the correct causal association is rarely confirmed.
Although several hypotheses indicate a possible involvement of EMRFR in the onset or worsening of tinnitus, this relationship has not been well-established and the mechanism by which it would happen remains unclear.17
The objective of this study was to perform a systematic review of the current knowledge on tinnitus and exposure to EMRFR, analyzing the evidence on their possible relationship.
MethodsIt was aimed to conduct the study as close as possible to a systematic review, although the objective (evaluating evidence of possible causal associations between tinnitus and exposure to electromagnetic radiofrequency radiation) differs from the typical objective of systematic reviews (evaluating evidence from randomized clinical trials with regard to a particular intervention).
A careful literature review was performed in the PubMed database between May and June of 2014, searching for the following descriptors: tinnitus AND electromagnetic field (144 results), tinnitus AND cell phones (11 results), tinnitus AND radiofrequency (eight results), tinnitus AND electromagnetic hypersensitivity (two results). A total of 165 items were found and read. Afterwards, the 45 studies that demonstrated clinical significance in at least one of the subjects (tinnitus and electromagnetic radiation) or in the possible link established between them were selected.
Standards for regulation of exposure to EMRFR postulated by Brazilian National Telecommunications Agency (Agência Nacional de Telecomunicações) occupational levels and users18 were also analyzed.
A printed manuscript used to successfully argue against the deployment of cellular antennas in residential buildings was also included. Despite not having been published, it contains scientific references in agreement with the data found in PubMed, as well as standards for safe exposure to EMRFR.
ResultsFor clarity, the results of this review will be presented as items.
Exposure to electromagnetic radiation (EMR)EMR can be ionizing or non-ionizing. The latter does not produce ionization of molecules, but can cause electrical, chemical, and thermodynamic cell damage.19 Examples of this group are infrared, ultraviolet, laser, radiofrequency, and microwave radiation.
EMRFR consists of electromagnetic waves with frequencies between 3kHz and 300GHz,20 so a part of them can stimulate the auditory system. They are produced by natural or synthetic sources and may penetrate the exposed tissues. The rate of absorption of such energy depends on the power of the EMRFR and the tissue's characteristics. The absorbed rate is converted into heat.21 To measure the thermal effect of electromagnetic radiation on the human body, the specific absorption rate (SAR) is used, which is a measure of the power density per unit mass. The SAR quantifies the energy absorbed by the tissue, which is directly proportional to the local increase of temperature.19
International organizations have established limits for exposure to general sources of EMRFR. SAR values set by the International Commission on Non-Ionizing Radiation Protection (ICNIRP), an independent scientific organization based in Germany, formally recognized by the World Health Organization and adopted by ANATEL are:18,22
- •
Occupational limit: 0.4W/kg
- •
General public limit: 0.08W/kg
Specifically for cell phones, because they are used near to the head or body, the ICNRP determined that the local SAR should not exceed the average limit of 2W/kg in 10g of tissue.23 Those limits aim to prevent effects to human health and reflect the current state of knowledge. Thus, the SAR limits currently adopted were established primarily to prevent thermal effects related to increasing body temperature.23
Although cell phones have much lower thermogenic potential than the maximum limits, heating of ear skin (2.3–4.5°C) is a common complaint, as well as proven temperature rise in tympanic membrane (0.02°C). Such heating varies according to the device frequency and duration of use; the longer the contact duration between cell phone and the ear, the greater the expected heating. Data on increased brain temperature is still insufficient.15
In addition to the thermal effects, biological effects have also been discussed.24 A specific concern is possible EMRFR cell genotoxicity, which has been studied in human lymphocytes in six independents centers.25 The presence of chromosomal and micronuclear alterations was evaluated, but it was not possible to establish a relationship between EMRFR and genotoxicity.25
The current functions of cell phones, with the advent of smartphones, go beyond regular phone calls. The widespread use of 3G wireless and Bluetooth functions entails an additional concern for the auditory system. However, recent studies have not indicated adverse effects of Bluetooth on the auditory system.26,27
Although little damage has been demonstrated so far, the study of EMRFR effects on different organs and systems should remain of utmost importance in public health. Any proven harmful effect can have wide-ranging implications, due to the universal exposure to EMRFR.28 In addition, further research should always monitor the presence of possible harms in medium and long term.
In contrast, a study published29 in 1992 showed substantial evidence that when pre-exposed to low doses of DNA-damaging factors such as ionizing radiation, ultraviolet light, alkylating agents, and oxidants, cells can develop an adaptive response, with consequently greater resistance to higher doses of aggressive agents. The manner by which it occurs is not completely elucidated, but the role of the DNA's repair mechanism has been demonstrated,30 with active participation of protein p53.31 From the clinical point of view, this adaptive possibility might be one of the reasons why some patients are more sensitive and others are more resistant to the same degree of exposure to the same aggressive agents.
Tinnitus and EMRFR: the question of electromagnetic hypersensitivityVarious symptoms involving one or more organs on the same individual have already been related to the exposure to electromagnetic fields.32 Approximately 3%–5% of the population subjectively associates the presence of nonspecific symptoms to acute or subacute exposure to EMRFR, even at levels below the safe limit of exposure.33,34
These symptoms were generally referred to as electromagnetic hypersensitivity (EMH) or electrosensitivity.35 The term EMH can be used in two contexts:
- •
As the ability of some individuals to perceive or react to the presence of EMR at significantly lower levels than the majority of the population.
- •
As a medical condition based on the interpretation of the patients about their condition, independent of any established causal relationship.
EMH has been better detailed in European and Scandinavian countries, and it has been widely reported on the media.36 It is already accepted that EMH causes major impact on quality of life, increased use of health care, and psychosocial disorders,37 in addition to reduction of work capacity, unemployment, and early retirement in Scandinavian countries.38 Thus, some individuals already are aware to avoid exposure to EMR as much as possible.35 It is the authors’ opinion that, as in many other health issues, developing countries such as Brazil would benefit by following the steps of developed countries.
Although EMH has been related to individual characteristics and not to a mandatory variable of exposure to EMRFR, there is already evidence of the influence of EMRFR in cognitive function and neural processing in the auditory central cortex.39 It is suspected that EMH can be manifested as cognitive dysfunction, with reduced discrimination by the sensory system and increased cortical activation in the anterior cingulate gyrus and insula.40 If this hypothesis is correct, auditory involvement would have a causal basis.
Tinnitus has been reported as one of the symptoms in patients with EMH.37 In a case-control study involving 89 patients with EMH and 107 controls matched by sex, age, and exposure to common sources of EMRFR, tinnitus prevalence was significantly higher in patients with EMH (50.72% vs. 17.5%).17
From this standpoint, it has been attempted to find factors that corroborate the relationship between tinnitus and EMH. One factor repeatedly observed in patients with EMH is reduction in the ability to discriminate magnetic pulses, which had already been identified as a predictor of tinnitus.41 Furthermore, tinnitus and EMH seem to share similarities in pathophysiology related to sensory discrimination.
Another common point is the vulnerability of patients with EMH to distress agents, affecting the autonomic nervous system (ANS).42 The state of ANS hyperexcitability may be mediated by changes in cortical glutamatergic receptors, which can be responsible for a decreased adaptive capacity in these individuals.43 Besides this, ANS hyperexcitability during the onset and worsening of tinnitus is well known.44
However, despite the significantly greater occurrence of tinnitus in patients with EMH, Landgrebe et al.17 found no association between tinnitus and individual exposure to EMRFR, suggesting that this exposure does not appear to cause tinnitus directly. This finding can be countered by other evidence, though. It has been shown that intensive use of cell phone and use for prolonged periods (≥4 years) are associated with tinnitus,45 suggesting that this device should be studied as a potential risk factor. Furthermore, as the prevalence of tinnitus has been rising worldwide,2 importance of environmental factors in tinnitus inception should be considered.
DiscussionCurrent scientific research has increasingly fast development. The universal motivation for conducting research in academic centers and the increasing availability of scientific journals have contributed to the globalization of expertise. However, only a small portion of published scientific articles reach a level of evidence sufficiently convincing to most researchers.
In the present study, although the authors found little statistically significant evidence of the influence of EMRFR on tinnitus, the association between these conditions should not be neglected, either.
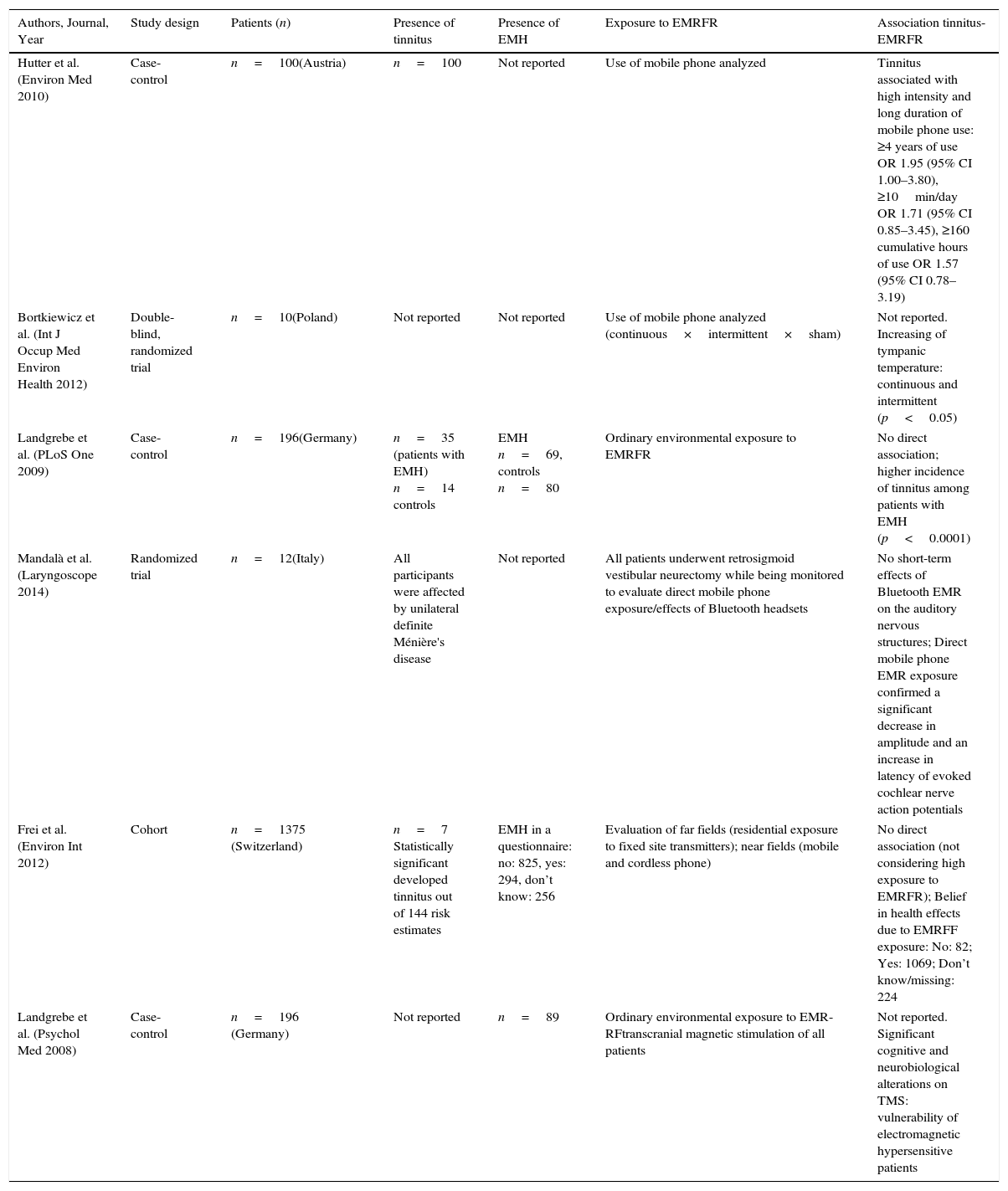
The main studies that evaluated tinnitus, exposure to EMRFR, and presence of EMH are compared on Table 1.
Comparison of the extracted data from the main articles of the present review.
| Authors, Journal, Year | Study design | Patients (n) | Presence of tinnitus | Presence of EMH | Exposure to EMRFR | Association tinnitus-EMRFR |
|---|---|---|---|---|---|---|
| Hutter et al. (Environ Med 2010) | Case-control | n=100(Austria) | n=100 | Not reported | Use of mobile phone analyzed | Tinnitus associated with high intensity and long duration of mobile phone use: ≥4 years of use OR 1.95 (95% CI 1.00–3.80), ≥10min/day OR 1.71 (95% CI 0.85–3.45), ≥160 cumulative hours of use OR 1.57 (95% CI 0.78–3.19) |
| Bortkiewicz et al. (Int J Occup Med Environ Health 2012) | Double-blind, randomized trial | n=10(Poland) | Not reported | Not reported | Use of mobile phone analyzed (continuous×intermittent×sham) | Not reported. Increasing of tympanic temperature: continuous and intermittent (p<0.05) |
| Landgrebe et al. (PLoS One 2009) | Case-control | n=196(Germany) | n=35 (patients with EMH) n=14 controls | EMH n=69, controls n=80 | Ordinary environmental exposure to EMRFR | No direct association; higher incidence of tinnitus among patients with EMH (p<0.0001) |
| Mandalà et al. (Laryngoscope 2014) | Randomized trial | n=12(Italy) | All participants were affected by unilateral definite Ménière's disease | Not reported | All patients underwent retrosigmoid vestibular neurectomy while being monitored to evaluate direct mobile phone exposure/effects of Bluetooth headsets | No short-term effects of Bluetooth EMR on the auditory nervous structures; Direct mobile phone EMR exposure confirmed a significant decrease in amplitude and an increase in latency of evoked cochlear nerve action potentials |
| Frei et al. (Environ Int 2012) | Cohort | n=1375 (Switzerland) | n=7 Statistically significant developed tinnitus out of 144 risk estimates | EMH in a questionnaire: no: 825, yes: 294, don’t know: 256 | Evaluation of far fields (residential exposure to fixed site transmitters); near fields (mobile and cordless phone) | No direct association (not considering high exposure to EMRFR); Belief in health effects due to EMRFF exposure: No: 82; Yes: 1069; Don’t know/missing: 224 |
| Landgrebe et al. (Psychol Med 2008) | Case-control | n=196 (Germany) | Not reported | n=89 | Ordinary environmental exposure to EMR-RFtranscranial magnetic stimulation of all patients | Not reported. Significant cognitive and neurobiological alterations on TMS: vulnerability of electromagnetic hypersensitive patients |
EMH, electromagnetic hypersensitivity; EMRFR, electromagnetic radiofrequency radiation; n, number; OR, odds ratio; CI, confidence interval; TMS, transcranial magnetic stimulation.
Even so, the advance of rigorous science itself has shown that well-established opinions change over time as new data are incorporated into the research. It is widely accepted that evidence-based medicine should inspire and guide professional conduct. However, the opposite is also true: anecdotal cases seen in the daily routine should also inspire science to deepen knowledge and confirm the existence or the reproducibility of the facts, considering that many studies are needed to form critical opinions. Publications of case reports, for example, are undervalued by the scientific community, but still have an important role to warn about facts that could be widely accepted later.
With this in mind, for years the authors have observed patients with tinnitus considered idiopathic, even after investigating multiple etiologies listed in the medical and audiological protocol. Emphasizing the suspicion of the patients, the authors included the questions about exposure to non-ionizing radiofrequency electromagnetic radiation in the diagnostic routine:
- 1.
Vicinity (residence or business) to towers, antennas, and transmission lines
- 2.
Use of the cell phone for calls:
- •
Approximate daily time of use
- •
Type of normal use: direct contact with the ear, headset, or Bluetooth
- •
Preferential use in one of the ears
- •
Adopting these extra data, it was easier to suspect the influence of EMRFR on tinnitus due to frequent cell phone use, especially in cases of prolonged use, with the preferred ear coinciding with the presence of unilateral (or worse) tinnitus. These are the patients who might be more vulnerable to have electromagnetic hypersensitivity (EMH) or electrosensitivity.
The peripheral auditory pathway has the ability to capture sound waves from the environment and transmit them actively to the cortex. Since EMRFR also presents diverse frequencies (starting at 3kHz) and amplitudes, similar to that which occurs with sound waves, it is plausible to accept that certain frequencies and amplitudes of EMRFR can be captured by the peripheral auditory system. Valid comparison is made to skin, another sense organ, responsible for capturing thermal, tactile, and painful sensations, which can be highly affected by infrared radiation.
Although cell phone manufacturers ensure that their use is safe, the World Health Organization has classified radiofrequency electromagnetic radiation as a potential carcinogen (class 2B), the same classification used for lead, chloroform, and emissions from automobiles. This warning was based on the analysis of studies performed by 30 researchers from 14 countries, which suggest increased risk of gliomas and neuromas in cell phone users.46
The present review of the literature was purposely focused on tinnitus and has found interesting arguments about the possible relationship between this symptom and EMRFR. However, due to multiple neuronal mechanisms involved in the pathogenesis of each one, whether there is a causal association between EMH and tinnitus, whether EMH is a predisposing factor for the worsening of tinnitus, or whether both share a similar pathophysiology is still under discussion.17 Prospective cohort studies will define more precisely if the risk of onset of tinnitus is higher in cell phone users or those with other sources of radio frequency exposure.
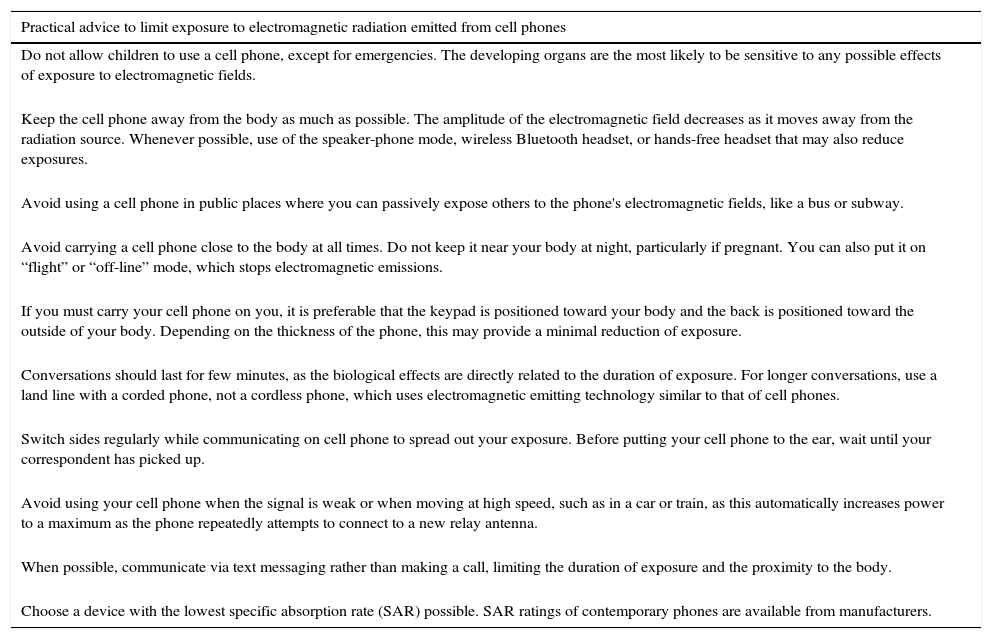
In the history of science, a long time is often necessary to gather enough conclusive studies to support opinions on the exposure factor and risk of disease, i.e., as currently accepted on tobacco's effect upon various organs. As the cell phone has led to a great advance in communication in modern societies, and should remain so, the authors recommend the conduct of common sense related to its usage. Practical suggestions have been published by the University of Pittsburgh Cancer Institute47 (Table 2).
Suggestions for safe use of cell phones, according to the University of Pittsburgh Cancer Center, 2008.
| Practical advice to limit exposure to electromagnetic radiation emitted from cell phones |
|---|
| Do not allow children to use a cell phone, except for emergencies. The developing organs are the most likely to be sensitive to any possible effects of exposure to electromagnetic fields. |
| Keep the cell phone away from the body as much as possible. The amplitude of the electromagnetic field decreases as it moves away from the radiation source. Whenever possible, use of the speaker-phone mode, wireless Bluetooth headset, or hands-free headset that may also reduce exposures. |
| Avoid using a cell phone in public places where you can passively expose others to the phone's electromagnetic fields, like a bus or subway. |
| Avoid carrying a cell phone close to the body at all times. Do not keep it near your body at night, particularly if pregnant. You can also put it on “flight” or “off-line” mode, which stops electromagnetic emissions. |
| If you must carry your cell phone on you, it is preferable that the keypad is positioned toward your body and the back is positioned toward the outside of your body. Depending on the thickness of the phone, this may provide a minimal reduction of exposure. |
| Conversations should last for few minutes, as the biological effects are directly related to the duration of exposure. For longer conversations, use a land line with a corded phone, not a cordless phone, which uses electromagnetic emitting technology similar to that of cell phones. |
| Switch sides regularly while communicating on cell phone to spread out your exposure. Before putting your cell phone to the ear, wait until your correspondent has picked up. |
| Avoid using your cell phone when the signal is weak or when moving at high speed, such as in a car or train, as this automatically increases power to a maximum as the phone repeatedly attempts to connect to a new relay antenna. |
| When possible, communicate via text messaging rather than making a call, limiting the duration of exposure and the proximity to the body. |
| Choose a device with the lowest specific absorption rate (SAR) possible. SAR ratings of contemporary phones are available from manufacturers. |
This study collected evidence for the association between exposure to EMRFR and tinnitus in some patients, particularly those suffering from electromagnetic hypersensitivity. While it is not fully confirmed, the authors consider it appropriate to direct more attention to cell phone use in the diagnostic investigation of patients with hearing disorders, especially tinnitus.
Conflicts of interestThe authors declare no conflicts of interest.
The authors would like to thank the librarian Mr. Adilson Montefusco and in particular Mr. Soter Marcello Correa da Silveira for the vast material provided.
Please cite this article as: Medeiros LN, Sanchez TG. Tinnitus and cell phones: the role of electromagnetic radiofrequency radiation. Braz J Otorhinolaryngol. 2016;82:97–104.


