

Caudal septal dislocation is a respiratory and cosmetic problem. The correction of caudal septal dislocation is a challenging issue. Although different modalities have been described for the treatment, it is still controversial.
ObjectivesThis study aims to describe a two-level suture technique which can be used to correct and stabilize the septum in the columellar pocket.
MethodsThe caudal septum was fixed to the nasal spine with suturing, and an anterior columellar pocket was formed. Two septocolumellar sutures including superior and inferior were performed to correct the dislocated caudal septum and to increase the stability of caudal septum in the columellar pocket.
ResultsAnterior rhinoscopy showed no recurrent deviation or dislocation in our patients.
ConclusionOur suture technique is an effective and easy-to-use method to correct the caudal septal dislocation. It can also be used to increase the stability of corrected septum by other techniques. A two-level suture technique increases the success of correction and reduces the risk of postoperative septal caudal luxation, stabilizing the superior portion of the caudal septum, in particular. Therefore, it would reduce the rate of redo surgeries.
O desvio septal caudal é um problema respiratório e estético, e a sua correção é tarefa desafiadora. Embora tenham sido descritas diferentes modalidades para o tratamento, esse é ainda um tópico controverso.
ObjetivosO presente estudo objetivou descrever uma técnica de sutura em dois níveis, que pode ser empregada na correção e estabilização do septo na bolsa columelar.
MétodoO septo caudal foi fixado à espinha nasal com suturas, após a realização de uma bolsa columelar anterior. Duas suturas septocolumelares, superior e inferior, foram aplicadas para a correção do desvio septal caudal e, também, para maior estabilidade do septo caudal na bolsa columelar.
ResultadosRinoscopia anterior não resultou em recorrência do desvio ou luxação em nossos pacientes.
ConclusãoNossa técnica de sutura é um método efetivo e de fácil uso para a correção do desvio septal caudal. A técnica também pode ser utilizada para aumentar a estabilidade de septos corrigidos por outras técnicas. A técnica de sutura em dois níveis aumenta o sucesso da correção e diminui o risco de luxação septal caudal, estabilizando, em particular, a parte superior do septo caudal. Portanto, nossa técnica diminui o percentual de reoperações.
Correction of septal caudal dislocation is a challenging problem for both the surgeon and the patient. Septal fixation to the nasal spine is a primary method for stabilizing the caudal septum. However, it can be complicated for a surgeon with limited experience, while it can be unfeasible for the nasal spine resection, even for an experienced surgeon. Although it is stabilized, fixation can be inadequate due to damaged septal and nasal spine connections, thereby leading to postoperative luxation-induced re-deviation.1 In addition, insufficient support or over-resection may cosmetically produce loss of tip projection, columellar retraction, and supratip depression.1
The earliest and most common method for the correction of septal caudal dislocation is Metzenbaum's “swinging door” (SD) technique. Using this technique, dislocated caudal septum is shifted on the midline and fixed to nasal spine. In later years, Noorman published a modification of the SD technique which includes using maxillary crest as a doorstop after shifting of dislocated septum to the opposite side of dislocation.2 Another method was described by Goldman, in which cartilage scoring, resection and suturing steps were defined. Furthermore, the modified Goldman technique, which includes triangular cartilage resection from dislocated caudal septal cartilage and suturing steps was described by Lawson.3
Two different suture techniques, which can be used both to correct the caudal septal dislocation and as a complement to previous fixation of cartilage to nasal spine techniques by increasing the stability of caudal septum were published in the literature. Batioglu et al.4 described a caudal septal suture technique that can be used single or complementary to previous techniques, in which the caudal septum is sutured to the soft tissue between the medial crura of the lower lateral cartilages by incising the midpoint of the columella skin from outside with non-absorbable suture material. Kenyon et al.5 also described a technique that includes fixation of the dislocated caudal septum in the columellar pocket with midpoint mattress suture.
In this study, we aimed to describe an easy way to correct and increase the stability of the caudal septum in columellar pocket by suturing it in two-level, thus preventing re-dislocation of the caudal septum.
MethodsThis technique was performed between August 2010 and July 2014. Our suture technique was used in patients undergoing septoplasty due to mild to moderate septal caudal dislocation with or without nasal septal deviation of other parts of the nasal septum. A total of 71 patients who underwent septoplasty using the combined septocolumellar suture technique were enrolled. The study was approved by the Ethics in Research Committee of the institution, under protocol 2014/246.
Patients with septal caudal dislocation have been grouped as mild, moderate and severe depending on the degree of narrowing of the nares by dislocated caudal end of nasal septum. Dislocations narrowing the nares medially up to 25% were accepted as mild, from 25% to 50% as moderate, and over 50% as severe.
Routine preoperative and pre-anesthesia examinations were carried out. The surgical procedure was performed by a single surgeon on all patients. Following 0.05% of oxymetazoline hydrochloride administration to the nasal mucosa, lidocaine and 1/100,000 of adrenaline were infiltrated. A unilateral hemi-transfixion incision to the anterior portion of the nasal septum was performed. The incision was performed through the dislocated side of the septum and 2–3mm posterior to the cauda. Both mucoperichondrial flaps were elevated and an appropriate technique for septal pathology was applied. L-strut was preserved to maintain the structural function of the septum. The anterior septum was freed from all mucosal connections. Deviations of maxillary crest were corrected by excision or medial replacement. Of note, excess cartilage in the caudal septal base is resected. Other techniques including scoring, triangular cartilage resection or shifting the caudal septum to the opposite side of dislocation were carried out. A tunnel between the medial crus of the alar cartilages was created with angled converse scissors or curved iris scissors. The septum was initially re-attached to the maxillary spine through a 4.0 absorbable monofilament suture (Vicryl®, Ethicon Inc., USA).
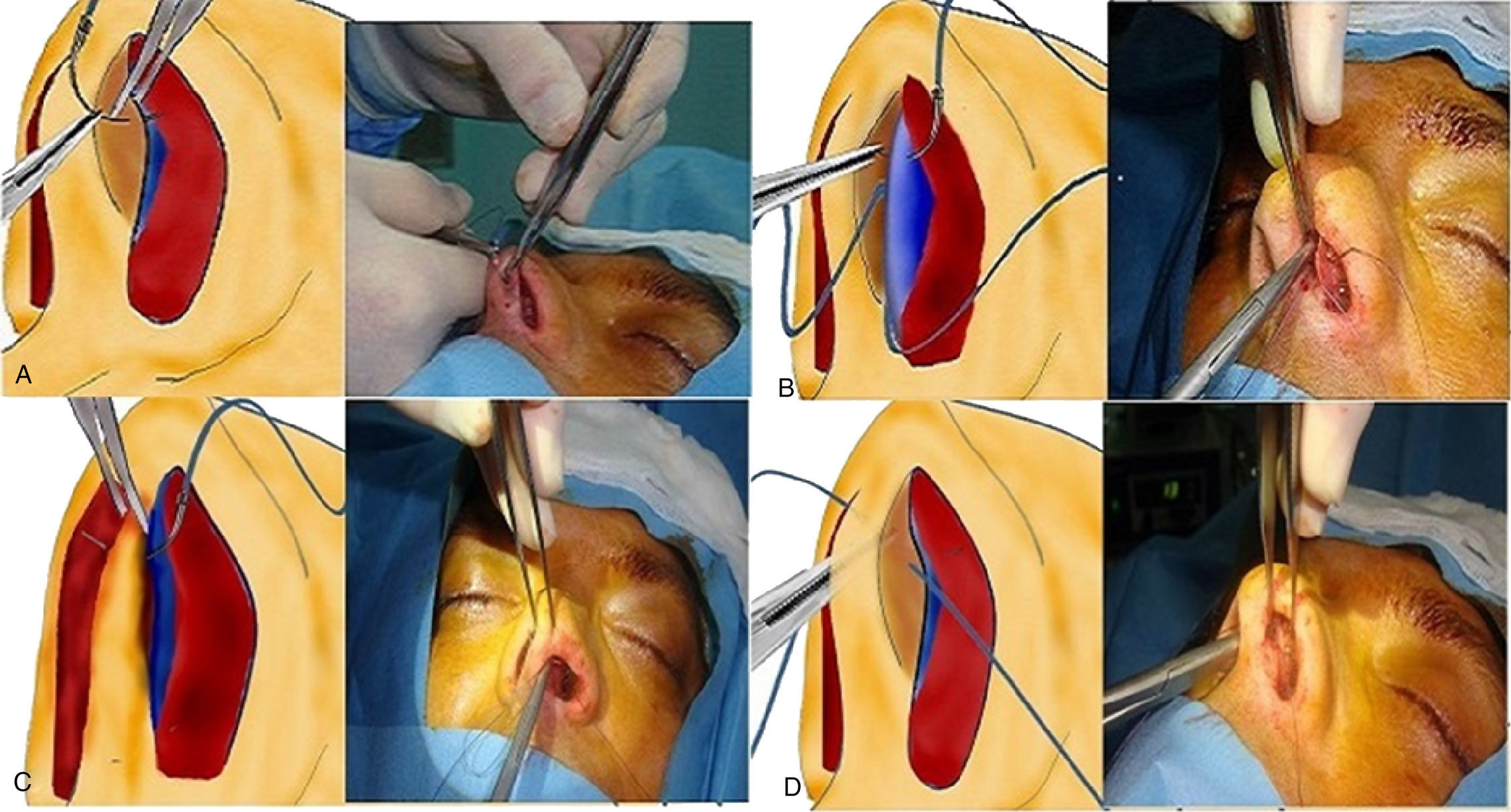
The cartilage was then prepared for superior septocolumellar suture with a 4.0 absorbable monofilament suture (Vicryl®, Ethicon Inc., USA). First suture was placed superiorly. The needle first passed through the alar cartilage of incision side from lateral to medial 3mm anterior to the mucoperichondrial incision (Fig. 1A). The needle was advanced through the septal cartilage (Fig. 1B). The needle passed through non-deviated, non-incised side mucoperichondrium from medial to lateral (Fig. 1C). Full-thickness was reinforced 2mm posterior of the mucoperichondrial incision, the needle was removed at the contra mucoperichondrium and it was, then, tied (Fig. 1D).

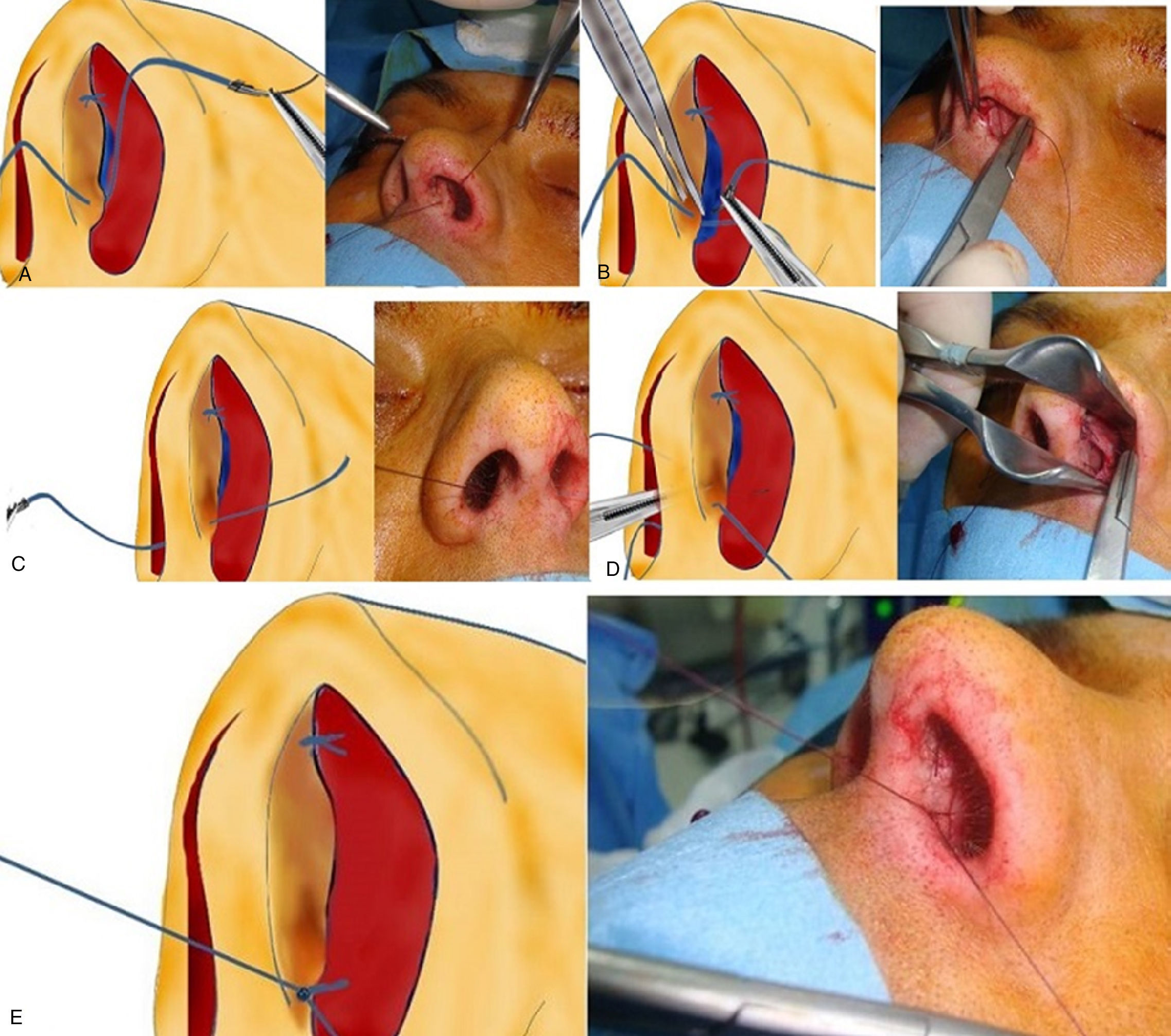
Inferior septocolumellar suturing was performed with a 4.0 absorbable monofilament suture (Vicryl®, Ethicon Inc., USA). The needle first passed through the alar cartilage of incision side from lateral to medial 3mm anterior to the mucoperichondrial incision (Fig. 2A). The needle was advanced through the septal cartilage (Fig. 2B). The needle passed through non-deviated, non-incised side mucoperichondrium from medial to lateral (Fig. 2C). Full-thickness was reinforced 2mm posterior of the mucoperichondrial incision, the needle was removed at the contra mucoperichondrium and it was, then, tied (Fig. 2D and E).

Internal Doyle silicon splints were left in place for 2 days in all cases.
ResultsWe performed this suturing technique on 71 septoplasty cases during four years. Among them, 44 (62%) were males and 27 (38%) were females. Total follow-up period ranged between 6 and 18 months. One patient (1.4%) had surgery-related bleeding. Anterior packing was replaced in this patient. Two patients (2.8%) had columellar indurations within the first week following surgery, resolved with antibiotic pomade. Anterior rhinoscopy showed no recurrent deviation or dislocation. Total follow-up duration was 6 months in 29 patients, one year in 23 patients, and 18 months in 19 patients. Preoperative (Fig. 3A) and sixth month postoperative (Fig. 3B) pictures of a patient operated with two level septocolumellar suture technique are seen.
Discussion
The nose, at the top of the respiratory system, is the most outwardly protruding and vulnerable part of the face. Therefore, it is the major organ which can be affected by maxillofacial injuries. Nearly 75–80% of the individuals had certain anatomical nasal deformities. Septoplasty is one of the major surgeries in the ear, nose, and throat practice. As the most involved area is the anterior part of the nose, septum should be robustly fixed during suturing at the end of surgery. Anterior septal deformity repair, in particular, is effective in preventing several complications including supratip depression, columellar retraction, and expansion of the nasal base.1 Although a successful surgery can be performed, insufficient fixation may yield undesirable outcomes. Our suture technique describes a way to fix caudal septum between two columellar cruras. It can be used additionally to SD or modified SD techniques.
In Metzenbaum's popular SD technique, dislocated caudal septum is shifted on the midline and fixed to nasal spine. In later years, Noorman modified SD technique by using maxillary crest as a doorstop after shifting of dislocated septum to the opposite side of dislocation.2 Both techniques are effective to correct caudal dislocations; however, they may be inadequate for selected cases or in cases in which maxillary spine must be removed and caudal septal fixation may not be adequate or sometimes impossible. Also, upper part of caudal septum tends to dislocate following the procedure due to insufficient support to this portion. In the present technique with a two-level fixation, stability increased and the risk for dislocation decreased. In the modified SD technique, on the other hand, caudal septum part removed from the other side of maxillary spine may narrow the airway passage. When combined with the SD technique, our suturing technique may yield to midway position of the caudal septum and equal airway passages.
The Goldman technique includes scoring, resection and suturing components, while the modified Goldman technique requires triangle shaped cartilage excision from the dislocated portion of caudal septum and suturing the septum to maxillary spine.3 These techniques may help to reduce nasal tip support and columellar retraction due to cartilage excision. In a study including 68 patients with caudal septal deviation, Batioglu et al.4 performed a point incision into the columellar midpoint following septoplasty and formed a columellar pocket. The incision was ceased using inside-to-outside suturing technique and carried out outside-to-inside suturing onto the midpoint incision site. Finally, the caudal tip of the septum was knotted in the columellar pocket. A 3.0 non-absorbable monofilament suture was used. They described dimple-shaped shrinkage on the columellar skin after the procedure. Although they report that this shrinkage disappeared within the first month and complete epithelization was achieved, this condition may become uncomfortable for the patient. In addition, as this technique includes a midpoint skin incision to columella, it may cause scarring. A non-absorbable suture material used in this technique may yield to suture material reaction in the long-term, even. Furthermore, burying the suture to soft tissue between medial cruras of the lower lateral cartilages may be challenging in unexperienced hands. Unless it is not performed alone, one-level fixation may not be sufficient to prevent re-deviation. Our technique uses absorbable suture materials without any skin incisions. Since it is performed layer by layer, it is very easy to learn and to perform. Two-level fixation may overcome the limitations of one-level fixation.
In another study, Kenyon et al.5 described mattress suture techniques in septal dislocation. A mattress suture in the incision site was used to fix the septum to open the full-thickness columellar pocket with a Kenyon suture technique. An absorbable suture such as 3.0 VicrlyRapide® was used. In this technique, septum is fixed in one level and mattress suture is performed through all three medial crura, septum, medial crura layers at one prick. However, it may be difficult to adjust the position of the caudal septum in the columellar pocket. In addition, it can only stabilize the septum vertically and when performed alone it may be inadequate for fixation, as it is a mattress suture and performed at one level. In our technique, backward movement of the needle was started 2mm posterior to first outward incision, thereby, horizontally stabilizing the septum. Furthermore, two-level suturing vertically fixates the caudal septum. We believe that layered advancing of the needle through the cartilages is easier even for inexperienced surgeons.
We did not perform nasal spirometry, acoustic rhinometry or radiological staging of nasal septal deviations to evaluate the severity of nasal septal deviation of the patients. It is a limitation to this study in objective patient selection. Because Mladina Classification6 does not give information about the severity of the septal caudal dislocation we did not use it in the selection of patients as mild or moderate. We selected patients as mild or moderate depending on inferior appearance of dislocated caudal septum. We used the degree of narrowing of the nares by the caudal end of dislocated septum. Patients accepted as severe caudal dislocation thought to be difficult to be evaluated by our technique and they were operated as open septoplasty or septorhinoplasty.
ConclusionIn conclusion, we suggest that two-level septocolumellar suturing is an effective and easy-to-use technique in the fixation of mild to moderate caudal septal deviations, supporting the nasal tip and preserving its symmetry. It does not require cartilage resection, thus preventing nasal tip support loss. In combination with the SD, modified SD, Goldman and modified Goldman techniques offer an advantage. Based on our current experience, it can yield considerable functional and cosmetic outcomes in the treatment of caudal septal dislocations. In addition, it is unlikely to lead to any scar or require septal support and it prevents nasal tip complications.
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Demirbilek N, Evren C, Elbistanlı MS, Altun U, Günay SS. Two-level septocolumellar suture technique for correction of septal caudal dislocation. Braz J Otorhinolaryngol. 2016;82:403–7.


