
Vestibular migraine (VM) is one of the most often common diagnoses in neurotology, but only recently has been recognized as a disease.
ObjectiveTo analyze the clinical and epidemiological profile of patients with VM.
MethodsThis was a retrospective, observational, and descriptive study, with analysis of patients’ records from an outpatient VM clinic.
Results94.1% of patients were females and 5.9% were males. The mean age was 46.1 years; 65.6% of patients had had headache for a longer period than dizziness. A correlation was detected between VM symptoms and the menstrual period. 61.53% of patients had auditory symptoms, with tinnitus the most common, although tonal audiometry was normal in 68.51%. Vectoelectronystagmography was normal in 67.34%, 10.20% had hyporeflexia, and 22.44% had vestibular hyperreflexia. Electrophysiological assessment showed no abnormalities in most patients. Fasting plasma glucose and glycemic curve were normal in most patients, while the insulin curve was abnormal in 75%. 82% of individuals with MV showed abnormalities on the metabolism of carbohydrates.
ConclusionVM affects predominantly middle-aged women, with migraine headache representing the first symptom, several years before vertigo. Physical, auditory, and vestibular evaluations are usually normal. The most frequent vestibular abnormality was hyperreflexia. Most individuals showed abnormality related to carbohydrate metabolism.
Migrânea vestibular (MV) corresponde a um dos mais frequentes diagnósticos em otoneurologia, o que justifica a importância de seu estudo, embora tenha sido apenas recentemente reconhecida como entidade nosológica.
ObjetivoAnalisar os perfis clínico e epidemiológico dos pacientes atendidos em um ambulatório de migrânea vestibular.
MétodoEstudo retrospectivo, observacional e descritivo, com análise de prontuários dos pacientes do ambulatório de MV.
ResultadosO ambulatório é composto por 94,1% de mulheres e 5,9% de homens, com média de idade 46,1 anos. O tempo de cefaleia foi superior ao de vertigem em 65,6% dos pacientes. Observou-se correlação entre os sintomas e o período menstrual. A maioria (61,53%) dos indivíduos apresentou algum sintoma auditivo, sendo o zumbido o mais frequente, embora a audiometria tenha sido normal em 68,51%. A vectoeletronistagmografia apresentou-se normal em 67,34%, enquanto 10,20% apresentaram hiporreflexia e 22,44% hiperreflexia vestibular. Exames eletrofisiológicos não mostraram alterações na maioria dos pacientes. Glicemia de jejum e curva glicêmica foram normais para a maioria dos pacientes, enquanto a curva insulinêmica mostrou-se alterada em 75% dos indivíduos. 82% dos indivíduos com MV apresentaram alguma alteração relativa ao metabolismo dos carboidratos.
ConclusãoMigrânea vestibular acomete, predominantemente, mulheres de meia idade, com cefaleia migranosa e vertigem, sendo a primeira de instalação mais precoce. O exame físico no período intercrise, bem como as avaliações auditiva e vestibular, mostram-se, geralmente, normais. O tipo de alteração vestibular mais observado foi a hiperreflexia labiríntica. A maioria os indivíduos avaliados apresentou alterações relativas ao metabolismo dos carboidratos.
The association between migraine and vestibular symptoms has been known for a long time, and became more evident after a systematic study carried out in 1984 by Kyan and Hood.1
Migraine and vertigo are common clinical conditions that affect, respectively, 14% and 7% of the general population. Their simultaneous occurrence would be 1%, if occurring at random. However, recent epidemiological studies indicate that 3.2% of the population have both migraine and vertigo.2,3 This can be attributed to two factors: vertigo syndromes (Meniere's disease, benign paroxysmal positional vertigo, and dizziness related to anxiety), which are more common in migraineurs when compared to controls; and vestibular migraine (VM).2–4
Vestibular migraine is an entity first described in 1999 by Dieterich and Brandt5 and corresponds to a variant of migraine whose main symptoms are vestibular. VM is more common in individuals without aura, and affects predominantly women, at a frequency of up to 5:1.4,6 Vestibular symptoms typically occur several years after the disease onset, when headache may be less frequent or even absent.2,4 The onset of vestibular symptoms replacing the headache is more commonly seen in perimenopausal women.7
The temporal association between migraine symptoms such as headache, photo and phonophobia, and the vestibular symptoms is variable, even in the same individual.6 VM episodes can be triggered by the same factors considered triggers for migraine headache, such as menstrual period, irregular sleep, stress, physical activity, dehydration, and certain foods and drinks, in addition to intense sensory stimulation.6,8
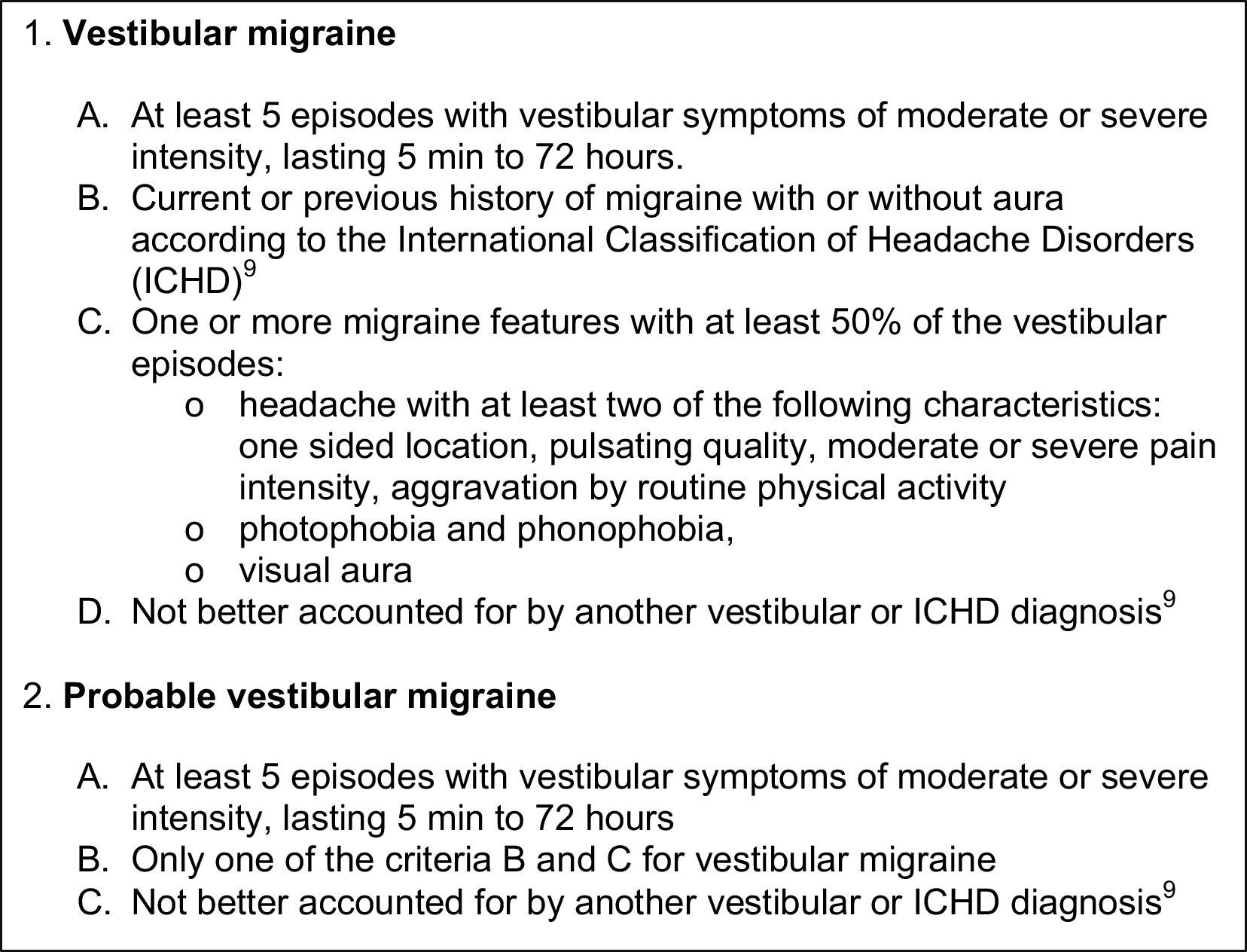
Diagnostic criteria for VM were proposed by Neuhauser in 20014 and revised in 2012 by Bárány Society, together with the International Headache Society, which included it in an appendix in 2013, of the third edition of the International Classification of Headaches, as a first step to identifying new entities (Figure 1).9,10
. 2014;170:401–6.")
The physical examination of patients with vestibular migraine is usually normal between crises. During disease episodes, however, there is often spontaneous or positional nystagmus, with characteristics of peripheral or central involvement.6,11 Vectoelectronystagmography is generally normal, with unilateral labyrinthine hypofunction reported in up to 20% of cases.6,12 Hearing assessment, likewise, is normal in most patients.6 Due to labyrinthine alterations, it is necessary to exclude other otoneurological diagnoses.
The aim of this study was to analyze the clinical and epidemiological profile of patients treated in the vestibular migraine outpatient clinic of the Otoneurology Service of the Discipline of Otology and Neurotology of the Department of Otorhinolaryngology and Head and Neck Surgery, Universidade Federal de São Paulo (UNIFESP).
MethodsThis was a cross-sectional, observational, and descriptive study, carried out at the vestibular migraine outpatient clinic of the Discipline of Otology and Neurotology of the Department of Otorhinolaryngology and Head and Neck Surgery of Universidade Federal de São Paulo (UNIFESP).
Patient records were selected from the VM outpatient clinic, since its creation in February of 2011 to June of 2013.
Patients were analyzed according to epidemiological data, such as gender, age, profession, and nationality, in addition to the clinical characteristics of the disease, previous medical history, and laboratory, auditory, and vestibular test results. This study was approved by the Research Ethics Committee of the Universidade Federal de São Paulo (UNIFESP) (No. 19615313.13.5.0000.5505).
Statistical tests were selected according to the data profile: the Kruskal–Wallis test was used to compare more than two variables, simultaneously; the Mann–Whitney test was used to compare variables in pairs; and the two-sample test for equality of proportions was used to assess whether the proportion of answers of two variables or levels was significant.
The 95% confidence intervals (95% CI) and p<0.05 were accepted for all analyses. SPSS v. 17, Minitab v. 16, and Excel Office 2010 were used for the statistical analysis.
ResultsOf the total of 85 patients, 80 (94.1%) were women and five (5.9%) were men, with ages ranging from 19 to 79 years – a mean of 46.1 years and a median of 47 years.
The time until symptom onset is shown in Figure 1. The symptom of headache appeared, on average, 7.3 years earlier when compared to dizziness. It was also observed that 65.6% of patients had had headaches for a longer period when compared to vertigo.
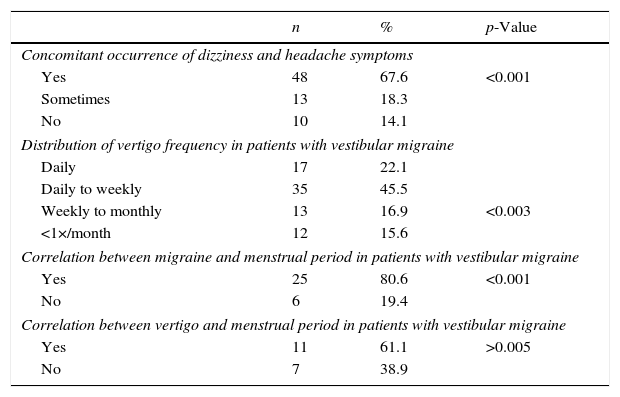
It was observed that headaches and dizziness occurred concomitantly in most patients, as shown in Table 1.
General aspects of symptoms in patients with vestibular migraine.
| n | % | p-Value | |
|---|---|---|---|
| Concomitant occurrence of dizziness and headache symptoms | |||
| Yes | 48 | 67.6 | <0.001 |
| Sometimes | 13 | 18.3 | |
| No | 10 | 14.1 | |
| Distribution of vertigo frequency in patients with vestibular migraine | |||
| Daily | 17 | 22.1 | |
| Daily to weekly | 35 | 45.5 | |
| Weekly to monthly | 13 | 16.9 | <0.003 |
| <1×/month | 12 | 15.6 | |
| Correlation between migraine and menstrual period in patients with vestibular migraine | |||
| Yes | 25 | 80.6 | <0.001 |
| No | 6 | 19.4 | |
| Correlation between vertigo and menstrual period in patients with vestibular migraine | |||
| Yes | 11 | 61.1 | >0.005 |
| No | 7 | 38.9 | |
Most patients experienced episodes of dizziness more often than once a week (Table 1).
Headache worsening during the menstrual period was reported by most female patients. The same could be observed in relation to dizziness, although it was not statistically significant (Table 1).
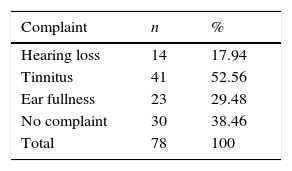
Forty-eight of 78 patients (61.53%) reported some auditory symptoms, and some reported more than one symptom (Table 2).
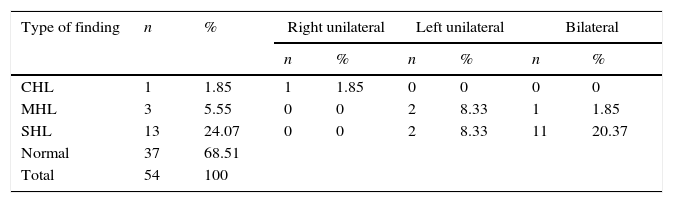
Fifty-four patients underwent tonal audiometry, which was normal in 37 (68.51%) individuals. Sensorineural hearing loss was the most frequently observed alteration (Table 3).
Pure tone audiometry findings in patients with vestibular migraine.
| Type of finding | n | % | Right unilateral | Left unilateral | Bilateral | |||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |||
| CHL | 1 | 1.85 | 1 | 1.85 | 0 | 0 | 0 | 0 |
| MHL | 3 | 5.55 | 0 | 0 | 2 | 8.33 | 1 | 1.85 |
| SHL | 13 | 24.07 | 0 | 0 | 2 | 8.33 | 11 | 20.37 |
| Normal | 37 | 68.51 | ||||||
| Total | 54 | 100 | ||||||
CHL, conductive hearing loss; MHL, mixed hearing loss; SHL, sensorineural hearing loss.
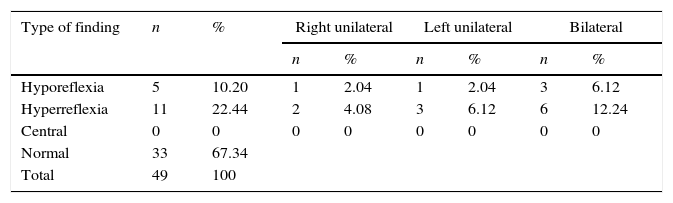
Vectoelectronystagmography was performed in 49 patients and was normal in most individuals. Among the changes, vestibular hyperreflexia was the most frequent, as shown in Table 4.
The brainstem evoked response audiometry (BERA) was shown to be altered in two (10.5%) of 19 patients who underwent the examination. In both, the alteration consisted of an increase in the electrophysiological threshold.
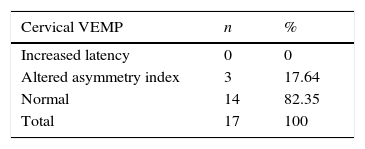
The cervical vestibular-evoked myogenic potential (VEMP) was assessed in 17 patients, and alterations were observed in three (17.6%) (Table 5).
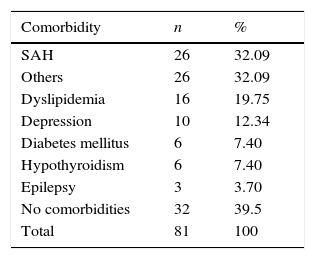
Of 81 patients, 49 (60.4%) had some comorbidity, among which systemic arterial hypertension (SAH) was the most prevalent (Table 6). Four records lacked this information.
Distribution of comorbidities in patients with vestibular migraine.
| Comorbidity | n | % |
|---|---|---|
| SAH | 26 | 32.09 |
| Others | 26 | 32.09 |
| Dyslipidemia | 16 | 19.75 |
| Depression | 10 | 12.34 |
| Diabetes mellitus | 6 | 7.40 |
| Hypothyroidism | 6 | 7.40 |
| Epilepsy | 3 | 3.70 |
| No comorbidities | 32 | 39.5 |
| Total | 81 | 100 |
SAH, systemic arterial hypertension.
Regarding the metabolic evaluation, glucose and insulin curves were requested for all individuals without a diagnosis of diabetes mellitus. For those known to be diabetics, fasting glucose measurement was requested.
Information on fasting glucose of 57 patients, with and without diabetes, was obtained. Of these, 71.92% showed normal and 28.08% had altered values (p<0.001). Values between 100 and 125mg/dL (impaired glucose tolerance) were observed in 21.75%, while 7.01% had fasting blood glucose greater than 125mg/dL (diabetes mellitus).13
Fifty-three patients, all without a prior diagnosis of diabetes mellitus, underwent the test after intake of 75g of dextrose. After 120min, 77.4% of the subjects had normal blood glucose levels (<140mg/dL and >55mg/dL); 22.6% had altered results (p<0.001) – 11.32% (n=6) showing decreased glucose tolerance (140–199mg/dL) and 5.6% (n=3) individuals had diabetes mellitus (blood glucose above 200mg/dL).13 Three individuals (5.6%) had glucose levels <55mg/dL (hypoglycemia) at 120min.13
Insulin curve was assessed in 43 patients, also without a diagnosis of diabetes mellitus. Of these, 74.5% had abnormal values, whereas 25.5% had normal results (p<0.001), according to the Kraft criteria.14,15 Hypoinsulinism (insulin <50μU/mL in all measurements) was observed in 17 (39.5%) individuals. The sum of the values at 120 and 180min was greater than 60μU/mL in seven (16.27%) patients (Kraft type II curve). The means of these values were, respectively, 64.3μU/mL and 23.4μU/mL.14,15 Eight tests showed delayed insulin peak, at 120 or 180min (Kraft type III curve).14,15
In total, 82.22% of the patients had some carbohydrate metabolism alteration, considering diabetes, hypoglycemia, decreased glucose tolerance, hypoinsulinism and occult diabetes, according to Kraft's criteria.
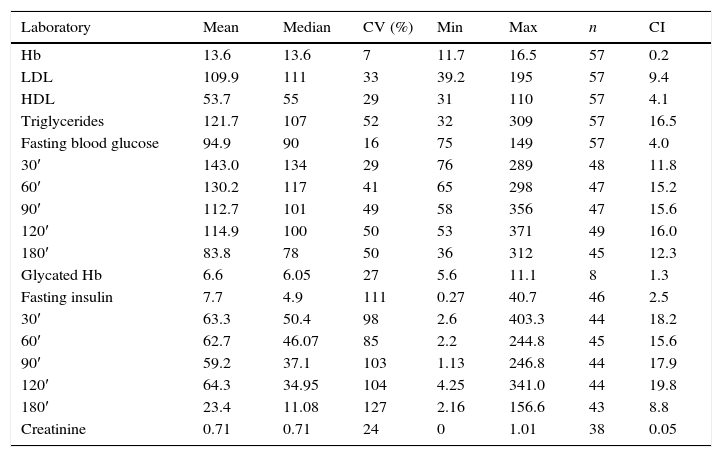
The mean values for glucose, insulin, hemoglobin, lipids, and creatinine are found in Table 7.
Metabolic assessment of patients with vestibular migraine.
| Laboratory | Mean | Median | CV (%) | Min | Max | n | CI |
|---|---|---|---|---|---|---|---|
| Hb | 13.6 | 13.6 | 7 | 11.7 | 16.5 | 57 | 0.2 |
| LDL | 109.9 | 111 | 33 | 39.2 | 195 | 57 | 9.4 |
| HDL | 53.7 | 55 | 29 | 31 | 110 | 57 | 4.1 |
| Triglycerides | 121.7 | 107 | 52 | 32 | 309 | 57 | 16.5 |
| Fasting blood glucose | 94.9 | 90 | 16 | 75 | 149 | 57 | 4.0 |
| 30′ | 143.0 | 134 | 29 | 76 | 289 | 48 | 11.8 |
| 60′ | 130.2 | 117 | 41 | 65 | 298 | 47 | 15.2 |
| 90′ | 112.7 | 101 | 49 | 58 | 356 | 47 | 15.6 |
| 120′ | 114.9 | 100 | 50 | 53 | 371 | 49 | 16.0 |
| 180′ | 83.8 | 78 | 50 | 36 | 312 | 45 | 12.3 |
| Glycated Hb | 6.6 | 6.05 | 27 | 5.6 | 11.1 | 8 | 1.3 |
| Fasting insulin | 7.7 | 4.9 | 111 | 0.27 | 40.7 | 46 | 2.5 |
| 30′ | 63.3 | 50.4 | 98 | 2.6 | 403.3 | 44 | 18.2 |
| 60′ | 62.7 | 46.07 | 85 | 2.2 | 244.8 | 45 | 15.6 |
| 90′ | 59.2 | 37.1 | 103 | 1.13 | 246.8 | 44 | 17.9 |
| 120′ | 64.3 | 34.95 | 104 | 4.25 | 341.0 | 44 | 19.8 |
| 180′ | 23.4 | 11.08 | 127 | 2.16 | 156.6 | 43 | 8.8 |
| Creatinine | 0.71 | 0.71 | 24 | 0 | 1.01 | 38 | 0.05 |
Hb, hemoglobin; LDL, low-density lipoprotein; HDL, high-density lipoprotein.
This cross-sectional study assessed the characteristics of patients with vestibular migraine. There was a higher prevalence among women, mainly between the fifth and sixth decade of life (mean 46.1 years), corroborating literature data.2–4,6 The later onset of vertigo symptoms, when compared to headache, was also confirmed.2,3,6
Dizziness appeared, on average, seven years after the pain onset. The worsening of headache during the menstrual period, well known among women diagnosed with migraine (50–60% of the cases), was also observed in the present sample.16,17 The same occurred with the correlation dizziness vs. menstrual period. However, for the latter, there was no statistical correlation, which may be due to the small sample size, or due to the onset of vertigo after menopause in many patients.6
Most patients reported concomitant occurrence of headache and vertigo, and isolated symptoms occurred in 14%. In these cases, migraine equivalents such as photo and phonophobia or aura must accompany vestibular episodes in at least 50% of the episodes in order to characterize VM. Otherwise, it can be defined as probable vestibular migraine.4,9,10 It was found that 77% of the individuals reported episodes of VM more than once per week.
Auditory symptoms were observed in 61.53% of the subjects, with the tinnitus representing the main complaint. However, the auditory assessment by pure tone audiometry was unaltered in 68.51% of patients. Hearing loss, when present, was predominantly sensorineural, bilateral, symmetric, descending, and mild. Similar findings were reported by Radtke et al., who attributed to VM a much slower hearing loss when compared to that observed in Meniere's disease.18
Vestibular assessment through vectoelectronystagmography was, in most cases, normal, in accordance with literature findings.6,18 The most frequently observed alteration, however, was bilateral vestibular hyperreflexia, followed by unilateral hyperreflexia. Some authors have mentioned unilateral labyrinthine hypofunction as the most frequent alteration.6,18 Radtke et al. found 16% unilateral hypofunction, 4% bilateral hyporreflexia, and the same value for bilateral hyperreflexia after a follow up of nine years.18
Regarding the electrophysiological assessment, both the BERA and VEMP were normal in most individuals.
A higher prevalence of hypothyroidism was found in this sample (7.4%) when compared to the Brazilian general population (1.5%)19 (p<0.001). For all other assessed comorbidities – hypertension, dyslipidemia, depression, diabetes, and epilepsy – there were no statistically significant differences.20–22
Most VM patients had normal fasting glucose, as well as normal values at 120min after administration of 75g of dextrose.13 However, the insulin curve showed an alteration in 75% of subjects.14,15
VM has been only recently described, and its diagnosis is purely clinical. The presence of symptoms that are common to other neurotological diseases, associated with the absence of an objective test, makes its diagnosis challenging.
Alterations in glycemic and/or insulinemic curves of individuals without a specific diagnosis can lead to overestimation of metabolic alterations as the primary cause of vestibular dysfunction. The error can also be supported by the good response of the individual to clinical treatment, which includes dietary recommendations and the practice of physical activities. It is known, however, that such measures are part of the first line of the prophylactic treatment of vestibular migraine, which could explain symptom improvement in patients who receive this kind of recommendation.
ConclusionVestibular migraine affects predominantly middle-aged women with a history of migraine headache and vertigo, with the first showing an earlier onset. Physical examination in the period between crises, as well as auditory and vestibular assessments, are usually normal. The most frequent vestibular alteration was labyrinthine hyperreflexia. Most of the assessed individuals had carbohydrate metabolism alteration.
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Morganti LOG, Salmito MC, Duarte JA, Bezerra KC, Simões JC, Ganança FF. Vestibular migraine: clinical and epidemiological aspects. Braz J Otorhinolaryngol. 2016;82:397–402.


