
Papillary carcinoma is the most common malignant thyroid neoplasm. The effect of the concurrent presence of Hashimoto's thyroiditis and papillary thyroid carcinoma remains controversial.
ObjectiveTo evaluate the association between Hashimoto's thyroiditis and clinicopathological parameters in thyroid papillary carcinoma cases, based on an historical institutional cohort analysis.
MethodsCross-sectional study obtained from a historical cohort, including all cases submitted to thyroidectomy for papillary thyroid carcinoma in a single institution during an 11-year period study.
ResultsA total of 417 patients with papillary thyroid carcinoma were enrolled; 148 (35.4%) also had Hashimoto's thyroiditis. A female predominance among cases associated to Hashimoto's thyroiditis was observed. The thyroid tumor, in cases associated with Hashimoto's thyroiditis, had a smaller mean diameter, lower frequency of extra-thyroid extension, and earlier clinicopathological staging.
ConclusionsA high proportion of papillary thyroid carcinoma cases are associated with Hashimoto's thyroiditis. There are associations among these cases with several histopathological factors already recognized for their prognostic value, which by themselves could impact outcomes.
O carcinoma papilífero é a neoplasia maligna mais comum da tireóide. O efeito da coexistência da tireoidite de Hashimoto (TH) no prognóstico do carcinoma papilífero da tireóide (CPT) permanece controverso.
ObjetivoAvaliar a associação entre TH e parâmetros clínico-patológicos entre pacientes com diagnóstico de carcinoma papilífero da tireóide obtidos através da análise de uma série histórica institucional.
MétodoCoorte transversal com base em uma coorte histórica, envolvendo todos os casos submetidos à tireoidectomia total por motivo de carcinoma papilífero, realizadas na mesma Instituição ao longo de 11 anos.
ResultadosUm total de 417 pacientes foram incluídos no estudo, estando 148 (35,4%) associados à TH. Observamos preponderância de mulheres entre os casos associados à TH. Esses casos se apresentaram com menor média de diâmetro tumoral, menor frequência de comprometimento extra-tireoidiano e estadiamento clínico-patológico mais precoce.
ConclusõesUm percentual expressivo de casos de CPT apresenta-se associado à TH. A associação entre esses casos, com vários fatores histopatológicos já reconhecidos por seu valor prognóstico, pode por sí só influenciar no desfecho desses pacientes.
Papillary thyroid carcinoma (PTC) and Hashimoto's thyroiditis (HT) are common diseases in clinical practice. Papillary carcinoma is the most common malignant neoplasm of the thyroid. HT is the most prevalent autoimmune disease and one of the most common endocrine diseases.1 This condition is the most common cause of hypothyroidism, excluding cases secondary to thyroidectomy, that are predominant among females.2 The association between PTC and HT was first described in 1955 by Dailey et al.,3 and became evident because of an increase in new cases of thyroiditis diagnosed by anatomopathological exams over the past decades. The concept of chronic inflammation as a risk factor for the development of malignancies has been well established for other tumors. However, with respect to these two entities, the association of cause and effect between them remains uncertain.4 Both diseases may have a subclinical course and may be merely an incidental diagnosis. Most publications on the subject are based on historical reviews of series of patients undergoing thyroidectomy, or on large exploratory studies among patients who underwent fine needle aspiration (FNA).4 The results now available do not allow definitive conclusions, although the evidence that nonspecific focal or multifocal lymphocytic infiltrates may also occur more frequently in cases of PTC suggests that the tumor can exert some degree of influence on the rest of the gland.1
Some authors have reported that the presence of HT in patients with PTC is associated with a less aggressive clinical presentation and course.5–7 However, other studies have not found similar effects.8–10 The objective of this study was to investigate a large institutional series of patients with PTC noting the prevalence of an association of HT and, comparing clinicopathological characteristics of PTC patients with or without an associated HT.
MethodsPatientsThe histopathological records of all patients who underwent total thyroidectomy at this institution with a final histopathological diagnosis of PTC from June of 2000 to December of 2010 were reviewed. Of 623 cases of thyroidectomy due to thyroid cancer conducted in the period, 417 (66.97%) met the inclusion criteria. All patients underwent clinical and ultrasonographic evaluation in the preoperative period. Relevant cases underwent cytologic evaluation of thyroid nodules by FNA. Neck dissection procedures in the central or lateral compartment are not performed electively at this institution, but rather are reserved for cases with clinical or ultrasonographic evidence of lymph node metastases. Patients with nonspecific focal (16 cases) or multifocal (40 cases) thyroiditis, cases of thyroid disease due to Graves’ disease (two cases) or xanthogranulomatous inflammation (four cases), cases submitted to partial thyroidectomy (60 cases), cases with more than one tumor histology in the same gland (two synchronous cases of papillary and follicular carcinoma, and one synchronous case of papillary and medullary carcinoma), and cases with no information on tumoral diameter (19 cases) were excluded from the analysis.
The following parameters were entered into a dedicated database (Microsoft Excel® 2003 version; Microsoft Corporation – Redmond, WA, United States): age, gender, concomitant HT, association with lymph node dissection, detailed histopathological description, predominant nodule diameter, multifocality, multicentricity, extra-thyroid extension, T, N, and M staging, and clinicopathological staging.
Definitions and pathologyIn this study, tumors were considered multifocal when two or more foci were found in the same lobe of the gland. Tumors were considered multicentric when the presence of more than one tumor focus in different lobes of the gland was found. The diagnosis of HT was based on histopathological findings. According to the study of Mizukami et al.,11 only cases with an association of lymphoplasmacytic infiltration with germinative center formation, oxyphilic cell metaplasia (Hürtle), atrophy, and fibrosis of thyroid follicles12 (also called signs of chronic oxyphilic lymphocytic thyroiditis) were classified as HT. Papillary microcarcinomata were defined as tumors with diameter ≤1.0cm at histological examination. The clinicopathological staging procedures were performed according to the American Joint Committee on Cancer TNM staging system (7th Edition).13 The lymph node status was defined by pathological evidence of metastasis in the lymph nodes that were removed. Extra-glandular involvement was determined based on evidence of tumor infiltrates beyond the gland capsule, at microscopic examination. All data were collected by the same researcher (Girardi FM) and all pathologic reviews were performed by the same pathologist (Barra MB).
Statistical analysis and ethical aspectsDescriptive analysis was used to summarize data. The Kolmogorov–Smirnov test was performed to assess the normality of continuous variables. Continuous variables with normal distribution were expressed as means and standard deviations. Those with non-normal distribution were also expressed as median and minimum–maximum values. Categorical variables were expressed as absolute and relative frequency. Student's t-test was used to compare means of age, the Mann–Whitney U test to compare tumor size, and the non-parametric chi-squared test for the comparison of categorical variables. This statistical analysis was performed using SPSS software version 15.0 (SPSS Inc. – Chicago, IL, United States). All tests considered a significance level of 5%.
The authors guarantee the preservation of data and the confidentiality of the material obtained. As no interventions were performed, an informed consent did not apply. This project was approved by the research ethics committee of this institution (Project No. 3483/11).
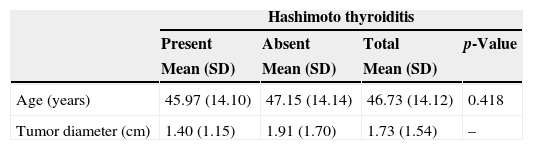
ResultsA total of 417 cases were included in this study, comprising 66.97% of the cases submitted to thyroidectomy for cancer at the institution from 2000 to 2010. Of this total, 339 (81.2%) were women. The male:female ratio was 1:4.3. The mean age was 46.73 (12.14) years, ranging from 13 to 87 years. In 148 (35.4%) cases, the patient harbored PTC together with HT. A statistically significant association of PTC with HT was observed, when compared to other histological subtypes (p<0.001). Patients with coexisting PTC and HT presented at an earlier clinicopathological stage and with a lower rate of extra-glandular involvement (Table 1). There was a predominance of females among cases associated with thyroiditis. This study did not observe statistically significant differences in the variable “age” between groups, nor with respect to multifocality, multicentricity, neurovascular invasion, and M staging. Similarly, no significant difference was found with respect to N staging, despite the higher frequency of cervical lymphadenectomy in the group with chronic lymphocytic disease.
Analysis of clinical and pathological characteristics according to the presence or absence of Hashimoto thyroiditis among cases of papillary thyroid carcinoma.
| Hashimoto thyroiditis | ||||
|---|---|---|---|---|
| Present | Absent | Total | p-Value | |
| Mean (SD) | Mean (SD) | Mean (SD) | ||
| Age (years) | 45.97 (14.10) | 47.15 (14.14) | 46.73 (14.12) | 0.418 |
| Tumor diameter (cm) | 1.40 (1.15) | 1.91 (1.70) | 1.73 (1.54) | – |
| Median (Min–Max) | Median (Min–Max) | Median (Min–Max) | p-Value | |
|---|---|---|---|---|
| Tumor diameter | 1.2 (0.04–6.5) | 1.3 (0.1–9) | 1.2 (0.04–9) | 0.007 |
| n (148) | % (35.4) | n (269) | % (64.5) | n (417) | % (100) | p-Value | |
|---|---|---|---|---|---|---|---|
| Women/men | 136/12 | 91.8/8.1 | 203/66 | 75.4/24.5 | 339/78 | 81.2/18.7 | <0.001 |
| Neurovascular invasion | 9 | 6.0 | 18 | 6.6 | 27 | 6.4 | 0.972 |
| Multifocality | 32 | 21.6 | 53 | 19.7 | 85 | 20.3 | 0.735 |
| Multicentricity | 54 | 36.4 | 78 | 28.9 | 132 | 31.6 | 0.143 |
| Extracapsular invasion | 33 | 22.2 | 96 | 35.6 | 129 | 30.9 | 0.006 |
| Lymphadenectomy | 79 | 53.3 | 102 | 37.9 | 181 | 43.4 | 0.003 |
| T stage | |||||||
| 1 | 98 | 66.2 | 126 | 46.8 | 224 | 53.7 | 0.002 |
| 2 | 12 | 8.1 | 31 | 11.5 | 43 | 10.3 | |
| 3 | 38 | 25.6 | 109 | 40.5 | 147 | 35.2 | |
| 4 | 0 | 0 | 3 | 1.1 | 3 | 0.7 | |
| N stage | |||||||
| 0 ou X | 115 | 77.7 | 200 | 74.3 | 315 | 75.5 | 0.240 |
| 1a | 23 | 15.5 | 37 | 13.7 | 60 | 14.3 | |
| 1b | 10 | 6.7 | 32 | 11.8 | 42 | 10.0 | |
| M stage | |||||||
| 0 | 148 | 100 | 267 | 99.2 | 415 | 99.5 | 0.755 |
| 1 | 0 | 0 | 2 | 0.7 | 2 | 0.4 | |
| Clinicopathological staging | |||||||
| I | 119 | 80.4 | 181 | 67.2 | 300 | 71.9 | 0.019 |
| II | 5 | 3.3 | 10 | 3.7 | 15 | 3.5 | |
| III | 22 | 14.8 | 63 | 23.4 | 85 | 20.3 | |
| IV | 2 | 1.3 | 15 | 5.5 | 17 | 4.0 | |
n, absolute frequency; %, relative frequency; SD, standard deviation; Min–Max, variation between minimum and maximum; p-value, level of significance used; multifocality, refers to more than one tumor focus in the same lobe; multicentricity, refers to the presence of bilateral disease.
The coexistence of HT and thyroid cancer has been reported several times in literature. Loh et al. found a strong association between PTC and lymphocytic thyroiditis6 – a finding consistent with other studies.2,5,14–16 In the present study, the prevalence of HT associated with PTC was 35.4%, a rate similar to that found in the study conducted by Kim et al.17 However, its influence on the behavior of thyroid carcinoma is still a matter of debate. Some studies reported a worse prognosis among cases associated with thyroiditis.18,19 Other investigations found a similar behavior among cases with or without associated thyroiditis.20 However, the majority of studies showed a protective effect of lymphocytic disease.5,6,14,21–25 Kashima et al. reported mortality and disease-free interval after ten years of 5% and 85% among patients without associated thyroiditis, compared to 0.7% and 95% among cases with association, respectively.5 The favorable outcome of these patients suggests that the association with thyroiditis may represent an anti-tumor response,26 although it is not clear whether the coexistence of both diseases is not simply a greater chance for a synchronous occurrence of two high-prevalence diseases. Loh et al. noted that the association with HT was associated with lower recurrence and mortality rates. In that study, the group with the higher recurrence rate showed a higher frequency of lymph node metastases, which may have contributed greatly to the rise in this rate. Even with the maintenance of statistical significance after the multivariate analysis of the association with good prognosis among cases affected by HT, the researchers of that study failed to elucidate the differences in aspects related to treatment between the two study groups. Moreover, the various subtypes of thyroid lymphocytic infiltrate were included. No one knows the exact prognostic influences of these subtypes, although it is known that they may represent the spectrum of manifestations of chronic lymphocytic thyroiditis.6 These methodological features were further explored in the study by Jeong et al., who also demonstrated a lower recurrence among cases associated with HT.27 However, both in that study and in others, the association with HT did not function as an independent predictor of a lower recurrence rate after a multivariate analysis.23,27
It is possible that the better prognosis of cases associated with HT simply arises from an association with other factors historically recognized for better prognoses, as has been observed among variants or tumor histopathological features.28 Kim et al. found a higher frequency of women, lower mean tumor diameter, and lower mean age among cases associated with HT.23 However, in another study, a higher frequency of bilateral disease among cases associated with HT was found, although its authors noted in the same patients, a greater rate of total thyroidectomy than in the control group.17 The present study observed a high prevalence of bilateral disease (31.6%), preponderant in the group associated with HT, although without statistical significance. Similar to the studies of Jeong et al. and Yoon et al., we found a lower mean tumor diameter and lower rate of extracapsular invasion among cases associated with HT.27,29 This set of variables, historically recognized by different prognostic steps, distinguish PTC cases associated with HT as a peculiar pattern of disease presentation.
Jeong et al. observed a greater number of lymph nodes resected among cases undergoing cervical lymphadenectomy in the group associated with signs of HT.27 Similarly, our study found a higher rate of cervical lymphadenectomy among cases associated with HT. In this service, cervical lymphadenectomies are performed only for cases with a clinical suspicion of PTC or with metastatic disease suggested by imaging studies. Since the rates of metastases did not differ between groups, as was observed by Jeong et al., this may suggest that, for some reason, possibly inflammatory factors, there are more clinically suspicious lymph nodes among patients with a diagnosis of HT.27
ConclusionsIn this study, we found a high prevalence of association between HT and PTC. The presence of HT was associated with disease presentation at an earlier stage and with factors historically recognized by better outcomes at the time of surgery, which could per se influence the prognosis and recurrence. However, to date, the finding of an association of HT with PTC should not modify the medical management; rather, this finding simply should draw the physician's attention to a peculiar pattern of disease presentation.
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Girardi FM, Barra MB, Zettler CG. Papillary thyroid carcinoma: does the association with Hashimoto's thyroiditis affect the clinicopathological characteristics of the disease? Braz J Otorhinolaryngol. 2015;81:283–7.
Institution: Complexo Hospitalar Santa Casa de Porto Alegre, Porto Alegre, Rio Grande do Sul, RS, Brazil.
gology tem o prazer em homenagear os revisores


