
Patients with vestibular hypofunction, a typical finding in peripheral vestibular disorders, show body balance alterations.
ObjectiveTo evaluate the postural control of patients with vertigo and unilateral vestibular hypofunction.
MethodThis is a clinical cross-sectional study. Twenty-five patients with vertigo and unilateral vestibular hypofunction and a homogeneous control group consisting of 32 healthy individuals were submitted to a neurotological evaluation including the Tetrax Interactive Balance System posturography in eight different sensory conditions.
ResultsFor different positions, vertiginous patients with unilateral vestibular hypofunction showed significantly higher values of general stability index, weight distribution index, right/left and tool/heel synchronizations, Fourier transformation index and fall index than controls.
ConclusionIncreased values in the indices of weight distribution, right/left and tool/heel synchronizations, Fourier transformation and fall risk characterize the impairment of postural control in patients with vertigo and unilateral vestibular hypofunction.
Pacientes com hipofunção vestibular, achado típico em vestibulopatias periféricas, apresentam alterações de equilíbrio corporal.
ObjetivoAvaliar o controle postural de pacientes vertiginosos com hipofunção vestibular unilateral.
MétodoTrata-se de um estudo clínico transversal. No total, 25 pacientes vertiginosos com hipofunção vestibular unilateral e um grupo controle homogêneo de 32 indivíduos hígidos foram submetidos à avaliação otoneurológica, incluindo a posturografia do Tetrax Interactive Balance System em oito diferentes condições sensoriais.
ResultadosO grupo experimental apresentou valores significantemente maiores do que o grupo controle quanto ao índice de estabilidade geral, índice de distribuição de peso, índice de sincronização da oscilação postural direita/esquerda e dedos/calcanhar, faixas de frequência de oscilação postural (F1, F2–F4, F5–F6, F7–F8) e índice de risco de queda, em diferentes condições sensoriais.
ConclusãoAlterações de distribuição de peso, sincronização da oscilação postural direita/esquerda e dedos/calcanhares, faixas de frequência de oscilação postural e do índice de risco de queda caracterizam o comprometimento do controle postural em pacientes vertiginosos com hipofunção vestibular unilateral.
One of the most important tasks of the human postural control system is the body balance on the small support base provided by the feet. The vestibular system, as a gravity sensor, is one of the main tools of the nervous system for the control of posture and balance when a person is standing and during locomotion. The difficulty to perceive movement, orient oneself vertically, control the position of the center of mass and stabilize the head result in gait and balance impairment.1
Problems of vestibular origin account for approximately 50% of the cases of body balance disorders, with dizziness being one of the most frequent complaints in specialized clinical offices. Thus, there is a strong impetus to evaluate labyrinthine function and identify possible vestibular lesions responsible for body balance impairment.2
The diseases that compromise the vestibular system are called vestibulopathies; peripheral ones comprise disorders of the inner ear (labyrinth) and/or the vestibular branch of the eighth cranial nerve; the central ones involve central nervous system vestibular nuclei, pathways and interconnections. The vestibulopathies are considered primary when they are the result of vestibular system structure dysfunction; and secondary when they are associated with clinical manifestations originating from other parts of the human body.3
The instability and postural imbalances of individuals with vestibular dysfunction usually manifest as increased body sway in situations of visual and somatosensory conflict, reduced stability threshold and functional capacity, a shifted gait and falls.4
A fall, the main result of postural imbalance, is a result of multiple factors. It can be defined as an unintentional displacement of the body to a level below the initial position due to an incapacity to promptly correct posture.5
Many neurotological evaluation methods have been developed to study body balance; the most commonly used procedures are the electronystagmography (ENG) and vecto-electronystagmography (VNG). Vestibular assessment performed with ENG or VNG is useful to substantiate or eliminate the diagnosis of vestibular involvement, locate the lesion at peripheral, central or a mixed level, establish the lesion prognosis, guide therapy and monitor evolution.6
The vestibular function tests can assess postural stability (vestibulospinal reflex or VSR) and vestibulo-ocular reflex (VOR); VOR is the primary control system for visual stabilization during locomotion and disturbances in this reflex result in dizziness and other symptoms of the loss of body balance.7
The evaluation of the VOR is insufficient to assess vestibular function as a whole. Although this reflex is essential for the body's angular displacement, the vestibulospinal reflex (VSR), visual and somatosensory information and sensory integration in the brain stem, actively participate in maintaining body balance, thus demonstrating the importance of a diagnostic method to assess this information.2
In clinical practice, postural stability is commonly assessed qualitatively by observing the static and dynamic balance. A quantitative evaluation can be performed using a posturography device consisting of a sensitive force platform that provides information about the patient's body sway.
Posturography measures the body sway and the variables associated with this sway. Posturography can be static, when it evaluates the subject's standing posture; and dynamic, when it measures the response to a disturbance applied to the subject.8
The posturography of the Tetrax Interactive Balance System (Tetrax™) is a diagnostic device developed by Reuven Kohen-Raz, in Israel, that analyzes the individual's postural balance and the mechanisms used to maintain it.9 This static posturography measures balance and postural sway on a platform consisting of four individual plates that capture variations in weight distribution.10 On each plate there is a strain gauge that converts the variations of the vertical forces into electrical signals of analog wave.9
The Tetrax™ allows the investigation of postural control through the difference in pressure on each platform and compares the values provided by the anterior and posterior portions of each foot (toes and heel) and of each heel with the anterior portion of the contralateral foot.9 The new parameters provided by the equipment may be useful in the clinical investigation of patients with balance disorders, undiagnosed through conventional tests.
In our country, the body balance of healthy individuals was assessed at the Tetrax™ in relation to the overall stability index, weight distribution index, left/right synchronization, toe/heel synchronization and risk of falls, in the following sensory conditions: eyes open and eyes closed and the head turned 45° to the right and to the left or tilted 30° forward and backwards, on a firm and unstable surface.11
The literature showed only one study that evaluated patients with vestibular dysfunction according to the Tetrax™ parameters, synchronization of sway between the toes and heels, weight distribution index on the four platforms (harmony in weight distribution) and intensity of low frequency sways, differentiating patients with normal ENG from patients with peripheral and central ENG; patients with normal caloric tests from those with caloric test alterations; and patients with right peripheral disorder from those with left peripheral disorder.12
The interest in quantifying and characterizing body balance in patients with vestibular dysfunction, a typical finding in peripheral vestibular disorders, and the scarcity of references on the Tetrax™ justified this study. The findings of Tetrax™, especially regarding the parameters that differ from those of other posturographies, may contribute to a more comprehensive knowledge of vestibular dysfunction in these patients, with potential diagnostic and therapeutic implications.
The aim of this research is to evaluate the postural control of patients with vertigo and unilateral vestibular hypofunction, through posturography using the Tetrax Interactive Balance System.
MethodThis clinical and cross-sectional study of a consecutive sample was initiated after approval by the Ethics Committee on Research with human subjects, number 1360-11. All volunteers were evaluated between 2011 and 2012 and were informed about the procedures that would be performed and signed the free and informed consent form to allow participation in the study and subsequent publication of the results.
A total of 25 patients with vertigo and unilateral peripheral vestibular dysfunction, who were of either gender and between 25 and 75 years of age, were enrolled. A control group, matched for age and gender with respect to the experimental group, consisted of 32 healthy volunteers from the community. Inclusion criteria for this group were absence of neurological diseases and body imbalance, with no history of vestibular and/or auditory symptoms, and a vestibular assessment by vecto-electronystagmography within the reference parameters.
Patients who had external and/or middle ear alterations, psychiatric disorders, history of otological surgery, were unable to understand and answer simple verbal commands, were unable to remain independently in the standing position, had severe visual impairment or were not compensated by the use of corrective lenses, orthopedic disorders that resulted in limited movement, needed lower-limb prosthesis and had undergone body balance rehabilitation in the last six months were excluded.
The patients were submitted to an evaluation consisting of clinical history, otorhinolaryngological examination, vestibular function and static posturography assessment.
The vestibular function assessment13,14 included positional and positioning nystagmus, spontaneous, semi-spontaneous, optokinetic nystagmus, fixed and randomized saccadic eye movements, pendular tracking, rotational chair testing and air caloric test at 50°C and 24°C at the VNG (digital vecto-nystagmograph VECWIN device, light bar and air caloric stimulator, Neurograff Eletromedicina Ind. e Com. Ltda – EPT).
Static posturography was performed using a Tetrax™ of Sunlight Medical Ltd., which includes a specific program installed on a computer, a platform consisting of four independent and integrated platforms (ABCD), placed on uncarpeted level ground with handrail and foam mat.
The patients placed the toes and heels on the four platforms (A, left heel; B, left toes; C, right heel; D, right toes) with the arms extended along the body and were instructed to remain in the standing position, stable and still for 32s in each of the eight sensory conditions: face forward, eyes open, looking at a target on the wall opposite to the platform, on a firm surface (NO); face forward, eyes closed, on a firm surface (NC); eyes closed, head rotated at 45° to the right, on a firm surface (HR); eyes closed, head rotated at 45° to the left, on a firm surface (HL); eyes closed, head tilted at 30° backwards, on a firm surface (HB); eyes closed, head tilted at 30° forward, on a firm surface (HF); face forward, eyes open, looking at a target on the wall opposite to the platform, on an unstable surface, on a cushion (PO); face forward, eyes closed, on an unstable surface, on a cushion (PC).
The Tetrax™ posturography evaluated the following parameters: stability index, weight distribution index, right/left and toe/heel synchronization index, frequency bands of postural sway (F1, F2–F4, F5–F6 tracks F7–F8) and fall risk.9
The stability index, regardless of weight and height, indicates the overall stability and the capacity to make postural changes. It assesses the amount of sway on the four platforms.9
The weight distribution index, expressed as percentage, is measured by comparing the deviations from the weight distribution on each platform in relation to a mean expected value of 25%.9
The synchronization index between the heel and the toes of each foot (AB, CD), between the two heels and the toes of both feet (AC, BD), between the heel of one foot with the contralateral foot toes (AD, BC), measures the coordination between the lower limbs and symmetry in weight distribution in each condition.9
The frequencies of postural sway, measured by Fourier Transformation, determine the intensity of postural sway within a variable spectrum between 0.01 and 3.0Hz. The Tetrax™ subdivides the spectrum of postural sway into four frequency bands: Low (F1) below 0.1Hz; Medium–Low (F2–F4), between 0.1 and 0.5Hz; Medium–High (F5–F6), between 0.5 and 1.0Hz; High (F7–F8) higher than 1.0Hz.9
The fall risk, expressed as a percentage and variable between zero and one hundred analyzes the results of the Tetrax™ parameters in the eight conditions. A value between 0% and 36% is considered as mild risk; a value between 37% and 58%, moderate risk; and between 59% and 100%, as high risk; the higher the score, the greater the risk of falls.9
All data were submitted to descriptive statistics for sample characterization. Levene's test was used to analyze the equality of variances regarding age and the Chi-square test to analyze the homogeneity of genders between the control and experimental groups. In the comparative analysis of the experimental and control groups, the nonparametric Mann–Whitney test was used when data distribution was asymmetrical; and the Student's t-test was used for independent samples, according to age, level of overall stability, weight distribution index, right/left and toes/heel synchronization index, postural sway frequency bands and fall risk in the eight sensory conditions. Data were shown as mean±standard deviation, median, minimum and maximum values. The level of significance was set at p<0.05. The Predictive Analytics Software (PASW, release 18.0) and MS Office Excel 2007 programs were used for the calculations.
ResultsA total of 57 individuals were evaluated, 25 from the experimental group consisting of patients with vertigo and unilateral vestibular hypofunction, of which 76% (n=19) were females and 24% (n=6) males and 32 in the control group, consisting of 62.5% (n=20) females and 37.5% (n=12) males. The mean age of the experimental group was 54.3±12.4 and the mean age of the control group was 55.9±13.4. The groups were homogeneous regarding gender (p=0.423) and age (p=0.752).
The experimental group had 12 subjects with right vestibular dysfunction (48%) and 13 subjects with left vestibular dysfunction (52%).
The risk of falls was moderate on average (mean±SD=50.4±38.8) in the experimental group and mild (mean±standard deviation=21.3±13.8) in the control group. The group with unilateral vestibular hypofunction showed a higher risk of falls than the control group, with statistically significant difference (p=0.001).
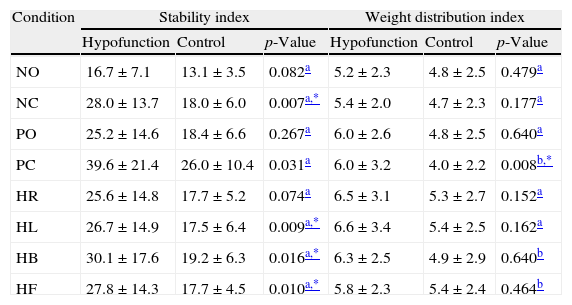
Table 1 shows a comparative analysis of the weight distribution index and stability index between the control group and the experimental group at the Tetrax™. The experimental group showed higher weight distribution index than the control group in all assessed conditions, with a statistically significant difference in the condition of eyes closed on an unstable surface. The experimental group showed higher stability index than the control group in all assessed conditions, with a statistically significant difference in the conditions of eyes closed on a firm surface (NC), head to the left (HL), head tilted backwards (HB) head tilted forward (HF) and eyes closed on an unstable surface (PC).
Analysis of the stability index and the weight distribution index in the eight conditions of the Tetrax Interactive Balance System (Tetrax™) in 32 control subjects and 25 patients with vertigo and unilateral vestibular hypofunction from the experimental group.
| Condition | Stability index | Weight distribution index | ||||
| Hypofunction | Control | p-Value | Hypofunction | Control | p-Value | |
| NO | 16.7±7.1 | 13.1±3.5 | 0.082a | 5.2±2.3 | 4.8±2.5 | 0.479a |
| NC | 28.0±13.7 | 18.0±6.0 | 0.007a,* | 5.4±2.0 | 4.7±2.3 | 0.177a |
| PO | 25.2±14.6 | 18.4±6.6 | 0.267a | 6.0±2.6 | 4.8±2.5 | 0.640a |
| PC | 39.6±21.4 | 26.0±10.4 | 0.031a | 6.0±3.2 | 4.0±2.2 | 0.008b,* |
| HR | 25.6±14.8 | 17.7±5.2 | 0.074a | 6.5±3.1 | 5.3±2.7 | 0.152a |
| HL | 26.7±14.9 | 17.5±6.4 | 0.009a,* | 6.6±3.4 | 5.4±2.5 | 0.162a |
| HB | 30.1±17.6 | 19.2±6.3 | 0.016a,* | 6.3±2.5 | 4.9±2.9 | 0.640b |
| HF | 27.8±14.3 | 17.7±4.5 | 0.010a,* | 5.8±2.3 | 5.4±2.4 | 0.464b |
Values are shown as mean±standard deviation.
NO, eyes open on a firm surface; NC, eyes closed on a firm surface; PO, eyes open on an unstable surface; PC, eyes closed on an unstable surface; HR, eyes closed with head rotation to the right on a firm surface; HL, eyes closed with head rotation to the left on a firm surface; HB, eyes closed; head tilted at 30° backwards on a firm surface; HF, eyes closed, head tilted forward at 30° on firm surface.
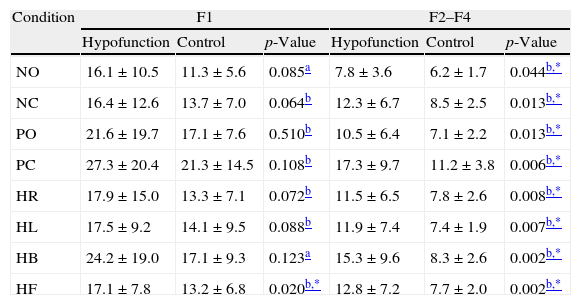
Table 2 shows the comparative analysis of the postural sway frequency bands (F1, F2–F4, F5–F6, F7–F8) in the control group and the experimental group in the eight sensory conditions of the Tetrax™. The group with unilateral vestibular hypofunction had higher values than the control group in all frequency bands. There was a statistically significant difference between groups in all postural sway frequency bands in the condition of eyes closed and head tilted forward (HF), in the bands F2–F4 and F5–F6 in the condition eyes open on a firm surface (NO) and in bands F2–F4, F5–F6 and F7–F8 in the other conditions.
Comparative analysis of Fourier frequency bands in the eight conditions of the Tetrax Interactive Balance System (Tetrax™) in 32 control subjects and 25 patients with vertigo and unilateral vestibular hypofunction in the experimental group.
| Condition | F1 | F2–F4 | ||||
| Hypofunction | Control | p-Value | Hypofunction | Control | p-Value | |
| NO | 16.1±10.5 | 11.3±5.6 | 0.085a | 7.8±3.6 | 6.2±1.7 | 0.044b,* |
| NC | 16.4±12.6 | 13.7±7.0 | 0.064b | 12.3±6.7 | 8.5±2.5 | 0.013b,* |
| PO | 21.6±19.7 | 17.1±7.6 | 0.510b | 10.5±6.4 | 7.1±2.2 | 0.013b,* |
| PC | 27.3±20.4 | 21.3±14.5 | 0.108b | 17.3±9.7 | 11.2±3.8 | 0.006b,* |
| HR | 17.9±15.0 | 13.3±7.1 | 0.072b | 11.5±6.5 | 7.8±2.6 | 0.008b,* |
| HL | 17.5±9.2 | 14.1±9.5 | 0.088b | 11.9±7.4 | 7.4±1.9 | 0.007b,* |
| HB | 24.2±19.0 | 17.1±9.3 | 0.123a | 15.3±9.6 | 8.3±2.6 | 0.002b,* |
| HF | 17.1±7.8 | 13.2±6.8 | 0.020b,* | 12.8±7.2 | 7.7±2.0 | 0.002b,* |
| Condition | F5–F6 | F7–F8 | ||||
| Hypofunction | Control | p-Value | Hypofunction | Control | p-Value | |
| NO | 3.3±1.5 | 2.6±0.8 | 0.043b,* | 0.4±0.2 | 0.4±0.1 | 0.266b |
| NC | 5.4±3.4 | 3.2±1.0 | 0.005b,* | 0.7±0.4 | 0.5±0.3 | 0.046b,* |
| PO | 4.7±2.8 | 3.6±1.4 | 0.005b,* | 0.7±0.4 | 0.6±0.1 | 0.046b,* |
| PC | 7.1±4.2 | 4.9±1.6 | 0.020b,* | 1.3±0.9 | 0.9±0.3 | 0.046b,* |
| HR | 4.9±2.8 | 3.3±1.0 | 0.012b,* | 0.7±0.5 | 0.5±0.2 | 0.047b,* |
| HL | 5.0±2.8 | 3.2±1.2 | 0.005b,* | 0.8±0.4 | 0.5±0.2 | 0.030b,* |
| HB | 5.4±1.2 | 3.5±3.4 | 0.013b | 1.0±0.6 | 0.6±0.2 | 0.012b,* |
| HF | 5.2±3.0 | 3.4±1.0 | 0.013b,* | 0.8±0.2 | 0.5±0.4 | 0.017b,* |
Values are shown as mean±standard deviation.
NO, eyes open on a firm surface; NC, eyes closed on a firm surface; PO, eyes open on an unstable surface; PC, eyes closed on an unstable surface; HR, eyes closed with head rotation to the right on a firm surface; HL, eyes closed with head rotation to the left on a firm surface; HB, eyes closed; head tilted at 30° backwards on a firm surface; HF, eyes closed, head tilted forward at 30° on firm surface.
F1, F2–F4, F5–F6; F7–F8, frequency bands of postural sway.
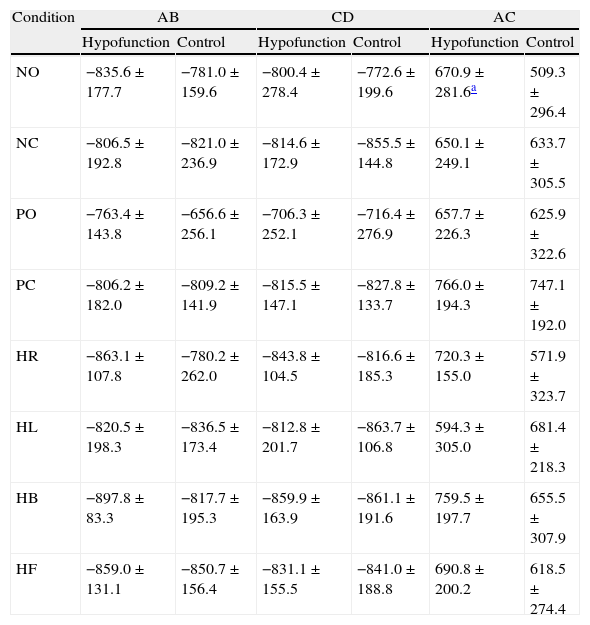
Table 3 shows the comparative analysis of the right/left and toes/heel synchronization index of the control group and the experimental group in the eight sensory conditions of the Tetrax™. There was no significant difference between the groups in the AB, CD, AC, BD, AD and BC (p>0.05) synchronizations in the conditions of eyes closed on a firm surface (NC), eyes closed and head turned to the right (HR), eyes closed and head turned to the left (HL), eyes closed and head tilted forward (HF), eyes open on an unstable surface (PO) and eyes closed on an unstable surface (PC).
Comparative analysis of indices of synchronization in the eight conditions of the Tetrax Interactive Balance System (Tetrax™) in 32 control subjects and 25 patients with vertigo and unilateral vestibular hypofunction from the experimental group.
| Condition | AB | CD | AC | |||
| Hypofunction | Control | Hypofunction | Control | Hypofunction | Control | |
| NO | −835.6±177.7 | −781.0±159.6 | −800.4±278.4 | −772.6±199.6 | 670.9±281.6a | 509.3±296.4 |
| NC | −806.5±192.8 | −821.0±236.9 | −814.6±172.9 | −855.5±144.8 | 650.1±249.1 | 633.7±305.5 |
| PO | −763.4±143.8 | −656.6±256.1 | −706.3±252.1 | −716.4±276.9 | 657.7±226.3 | 625.9±322.6 |
| PC | −806.2±182.0 | −809.2±141.9 | −815.5±147.1 | −827.8±133.7 | 766.0±194.3 | 747.1±192.0 |
| HR | −863.1±107.8 | −780.2±262.0 | −843.8±104.5 | −816.6±185.3 | 720.3±155.0 | 571.9±323.7 |
| HL | −820.5±198.3 | −836.5±173.4 | −812.8±201.7 | −863.7±106.8 | 594.3±305.0 | 681.4±218.3 |
| HB | −897.8±83.3 | −817.7±195.3 | −859.9±163.9 | −861.1±191.6 | 759.5±197.7 | 655.5±307.9 |
| HF | −859.0±131.1 | −850.7±156.4 | −831.1±155.5 | −841.0±188.8 | 690.8±200.2 | 618.5±274.4 |
| Condition | BD | AD | BC | |||
| Hypofunction | Control | Hypofunction | Control | Hypofunction | Control | |
| NO | 798.8±263.0a | 738.9±163.7 | −882.2±206.9a | −833.2±143.2 | −895.8±146.8a | −805.3±195.5 |
| NC | 808.4±141.8 | 846.6±107.8 | −899.7±70.3 | −864.9±163.3 | −913.3±52.9 | −884.3±110.5 |
| PO | 664.4±223.6 | 596.9±286.3 | −907.8±83.1 | −905.8±96.3 | −898.7±100.7 | −905.3±103.4 |
| PC | 757.4±184.4 | 785.0±139.7 | −937.5±45.5 | −939.9±47.8 | −943.6±41.8 | −933.1±66.7 |
| HR | 790.6±178.8 | 785.8±217.9 | −889.0±76.1 | −838.6±156.1 | −888.3±105.2 | −872.3±120.9 |
| HL | 821.5±142.2 | 803.9±167.1 | −871.8±75.3 | −874.2±125.3 | −872.9±99.9 | −875.7±125.3 |
| HB | 884.6±109.4a | 823.3±182.9 | −936.7±49.1a | −862.4±136.2 | −919.2±81.2 | −887.4±105.4 |
| HF | 839.5±92.9 | 822.9±181.6 | −905.9±58.6 | −864.0±116.0 | −904.6±61.9 | −851.8±159.5 |
Values are shown as mean±standard deviation.
AB, synchronization index between platforms regarding the left foot toes and heel; CD, synchronization index between the right foot toes and heel; AC, synchronization index between the two heels; BD, synchronization index between the two anterior parts of the foot; AD, synchronization index between the left heel and right toes; BC, synchronization index between the left toes and right heel; NO, eyes open on a firm surface; NC, eyes closed on a firm surface; PO, eyes open on an unstable surface; PC, eyes closed on an unstable surface; HR, eyes closed with head rotation to the right on a firm surface; HL, eyes closed with head rotation to the left on a firm surface; HB, eyes closed; head tilted at 30° backwards on a firm surface; HF, eyes closed, head tilted forward at 30° on firm surface.
Mann–Whitney test.
There was a statistically significant difference between groups, with higher values in the group of patients with vertigo and unilateral vestibular hypofunction, in the AC – right and left heels (p=0.020), BD – between right foot toes and left foot toes (p=0.018), AD – between the left heel and right foot toes (p=0.016) and BC – between left foot toes and right heel (p=0.011) synchronizations in the condition of eyes open on a firm surface (NO); in BD – between right foot toes and left foot toes (p=0.050) and AD – between the left heel and right toes (p=0.012) synchronizations in the condition of eyes closed and head tilted backwards (HB).
DiscussionThis study sought to evaluate body balance in an experimental group of patients with vertigo and unilateral vestibular hypofunction at the static posturography of the Tetrax™. This posturography uses different parameters and procedures from other types of posturographies, which makes the quantitative comparison of results difficult.
The fall risk in the experimental group showed significant increase, classified as moderate. We found no literature references on the fall risk at the static posturography of Tetrax™ in patients with vertigo and unilateral vestibular hypofunction.
The experimental group showed increased values of weight distribution index in the eight assessed conditions, but only significantly in the condition of eyes closed, on the cushion. These findings concur with reports that in situations of vestibular stress, as in the conditions of unstable surface and eyes closed, patients with peripheral vestibular disorders show significant worsening in weight distribution.12
As for the stability index, the experimental group showed an increase in all conditions evaluated, but significant only in the conditions of eyes closed on a firm surface; head turned the left, head tilted backwards, head tilted forward and eyes closed on an unstable surface. The values in the control group were within the reference parameters10 in all conditions, indicating little oscillation on the four plates and showing good overall stability. These results suggest that unilateral vestibular hypofunction compromises postural stability, mainly in situations involving visual information deprivation and proprioceptive information disturbance, similar to what was found when comparing a group of patients with dizziness and a control group.12
The experimental group showed a significant increase in values in all postural sway frequency bands in the condition of head tilted forward, in the bands F2–F4, F5–F6, and F7–F8 in the conditions eyes closed on a firm surface, head turned to the right, to the left, tilted backwards, eyes open on an unstable surface and eyes closed on an unstable surface and in the bands F2–F4 and F5–F6 in the condition of eyes open on a firm surface. Higher sway values were observed in the Low (F1) band and lower values in the Medium–High (F5–F6) and High (F7–F8) bands. The increase in the sway in the Medium–Low (F2–F4) band found in the experimental group is expected in peripheral vestibular dysfunction; the dominance of the sways in the Low (F1) band could indicate the influence of visual preference in postural control; dominant sways in the Medium–High (F5–F6) band would indicate somatosensory dysfunction and in the High (F7–F8) band, central vestibular dysfunction.9 We found no references in the literature on the frequency bands at the Tetrax™ static posturography in patients with vertigo and unilateral vestibular hypofunction.
The experimental group showed a significant increase in the synchronization index between the right heel and left heel (AC), right toes and left toes (BD), left heel and right toes (AD) and left toes and right heel (BC) in the condition eyes open on firm surface and in the synchronizations BD and AD in the condition head tilted backwards. The synchronization index values in the eight conditions were symmetric and positive or negative according to the expected in healthy individuals9 in the control and experimental groups, indicating coordination and synchronization. We found no literature references on the synchronizations indexes at the static posturography of the Tetrax™ in patients with vertigo and unilateral vestibular hypofunction.
The parameters evaluated by Tetrax™ were sensitive to demonstrate alterations in postural control mechanism in our patients with vertigo and vestibular hypofunction. In this research, the Tetrax™ provided relevant data on changes in the overall stability index, weight distribution index, right/left and toes/heel synchronization index postural sway frequency bands (F1, F2–F4, F5–F6, F7–F8) and fall risk in the assessment of postural control in patients with vertigo and unilateral vestibular hypofunction.
The identification of the characteristics of body balance disorders in patients with vertigo may have diagnostic, preventive and therapeutic implications. Further research should be undertaken to better clarify the consequences of alterations in these parameters on postural control and vestibular hypofunction, found in different neurotological clinical pictures.
ConclusionAlterations in weight distribution, right/left and toes/heels synchronization index, postural sway frequency bands and fall risk characterize postural control impairment in patients with vertigo and unilateral vestibular hypofunction, assessed by posturography of the Tetrax Interactive Balance System.
FundingThis study was supported by Coordenação de Aperfeiçoamento de
Pessoal de Nível Superior – CAPES.
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Quitschal RM, Fukunaga JY, Ganança MM, Caovilla HH. Evaluation of postural control in unilateral vestibular hypofunction. Braz J Otorhinolaryngol. 2014;80:339–45.
Institution: Escola Paulista de Medicina, Universidade Federal de São Paulo (UNIFESP-EPM), São Paulo, SP, Brazil.
gology is pleased to honor the reviewers


