


The use of Personal Digital Audio Players can cause hearing injuries, as the sound is generated directly in the ear canal. It is believed that different types of headphones can cause different amplifications, since they cause changes in the volume and resonance of the ear canal according to their depth.
ObjectiveThis study aimed to determine the sound pressure to which young individuals are exposed when using Personal Digital Audio Players with two types of headphones: insertion earphones and anatomical insertion earphones
Materials and methodsThis was an experimental study. The probe microphone measurements were made with different headphones in 54 ears (27 young individuals). The resonance peaks were also recorded.
ResultsA statistically significant difference was observed between the evaluated headphones, showing that anatomical insertion earphones had higher levels of sound pressure than insertion earphones for all frequencies measured. There was no correlation between the resonance peak of the closed canal and the frequency where the highest sound pressure level was obtained. There was a significant difference between ears at some frequencies with the different headphones.
ConclusionIt was concluded that anatomical insertion earphones generate a higher sound pressure level than insertion earphones.
© 2014 Associação Brasileira de Otorrinolaringologia e Cirurgia Cérvico-Facial. Published by Elsevier Editora Ltda. All rights reserved.
O uso de equipamentos portáteis sonoros individuais pode ser um risco auditivo, pois o som é gerado diretamente no meato acústico externo. Acredita-se que fones diferentes proporcionam amplificações diferentes, pois causam variações de volume e de ressonância conforme suas inserções.
ObjetivosVerificar a pressão sonora a que jovens estão expostos quando fazem uso de equipamentos sonoros portáteis individuais com dois diferentes fones: de inserção e de inserção anatômico.
Material e métodoTrata-se de uma pesquisa experimental. Para tanto, foram feitas medições em 54 orelhas de 27 jovens com idades entre 18 e 30 anos, com os dois tipos de fones. Também foram registrados picos de ressonância da orelha externa com e sem fone.
ResultadosObservou-se que o fone de inserção anatômico apresenta aumento do nível de pressão sonora estatisticamente significante em comparação com o fone de inserção para todas as frequências avaliadas. Não há uma correlação entre o novo pico de ressonância do meato fechado e a frequência na qual se obteve os maiores níveis de pressão sonora com o fone. Observou-se diferença estatisticamente significativa entre orelhas para algumas frequências com os diferentes fones.
Conclusãoo fone de inserção anatômico gera um maior nível de pressão sonora que o fone de inserção.
© 2014 Associação Brasileira de Otorrinolaringologia e Cirurgia Cérvico-Facial. Publicado por Elsevier Editora Ltda. Todos os direitos reservados.
Hearing is a sensory system of vital importance for humans who live in a society immersed in sounds and based on oral communication.
It is increasingly observed that the auditory system is exposed to high sound pressure levels, mainly by the changes in societal habits, such as venues where the sound is amplified, the use of sound equipment in cars, and the use of individual portable sound equipment, among others. Young individuals who, in today's society do not know how to live in silence and consider amplified sounds to be common and normal, are the segment of the population most exposed to amplified sounds.1
The technological revolution has greatly contributed to the acquisition of these new habits, launching new devices in the market that allow people to change their experiences. The technological developments that enable the amplification of sounds are a prime example. In the past, the radio was the only means of communication through which people learned the news. Over time this has evolved from portable radios so that today people can listen to the radio or to their favorite songs in any environment without affecting those around, as the sound comes from the the headphone and goes directly into the ear. This common attitude of listening to music at any time and any place characterizes the contemporary behavior.2
The technological revolution has been so comprehensive that it improved not only the equipment that allows for the transmission of sound signals, but also the the quality of the headphones, so that the signal suffers no distortion until it reaches the auditory system. However, the technological developments have also allowed many young individuals to listen to their sound equipment for long periods of time, at very high sound intensities, without considering whether this habit can harm the auditory system in the long term.
Many studies have shown that the use of individual portable sound equipment such as MP3 players and iPods can cause a reduction in the hearing thresholds of young individuals, as well as the early onset of auditory symptoms such as tinnitus and hearing problems.3-6
This concern affects everyone. Brazilian Law No. 11,291, of April 26, 2006,7 requires that manufacturers of individual portable sound equipment inform customers that hearing impairment may occur if the equipment is used above 85dB. Yet, more importantly than disclaimers in products, it is necessary that the users of these devices are aware of the risk they face.
The Brazilian Regulatory Standard 15 (RS 15),8 which addresses occupational medicine and safety, particularly the exposure of workers to noise, states that the maximum allowable daily noise exposure for exposure level of 85 dBA is eight hours. As an increase in sound intensity level occurs, the noise exposure time must decrease (for every 5dB increase, time is halved). Additionally, according to RS 15, individuals exposed to noise of 85 dBA must wear personal protective equipment (PPE) to protect their hearing. However, individual portable sound equipment can easily reach higher levels.
Studies have shown that such devices can reach up to 130dB, which is equivalent to the sound pressure level generated by a jackhammer. In context, the maximum allowed volume of 85dB corresponds to 65% of the total equipment capacity. Based on these studies9 and others, which state that almost 90% of the assessed young individuals use their equipment at maximum capacity,6 it is possible to infer that these young individuals exceed the recommended sound pressure levels and can damage their hearing.
Santos and Couto,10 in their study of young individuals, observed that they use their equipment on average for 1.83hours a day, at a mean volume of 70% of the total equipment capacity. However, this same study observed, through measurements with a probe microphone, that the average equipment can reach peaks of 100dB.
Specifically regarding the use of individual portable sound equipment, a question must be raised: does the type of headphone used favors greater amplification of the sound generated by the device? The use of headphones means that young individuals are at greater risk of exposure to high sound pressure levels, considering that the phone is inside the individual's ear, further amplifying the sound. Additionally, the sound pressure level is inversely proportional to the volume of the external ear, which, due to its shape, functions as a resonance tube.11
Therefore, the sound pressure levels that these devices emit, which are measured by decibelimeters, are actually higher when measured in the ear of the young individuals, near the tympanic membrane, as the ear canal amplifies the sound.12
Currently, earphones available in the market include external earphones, insertion earphones (IEs) that are made of rigid material and are located in the anterior portion of the external auditory meatus, and the anatomical insertion earphones (AIEs), which have a silicone tip, making them more flexible. The latter can be used more internally in the ear, preventing external sounds from interfering with the desired sound. Due to the insertion of this type of earphone inside the external auditory canal, there is probably a change in the volume of the external ear, causing the sound to be amplified more.11
Some studies,13 evaluating different types of headphones and the sound intensity they generate, observed that the output levels of IEs are on average 5.5dB higher than the output levels of supra-aural headphones when the environmental noise where the person is located increases. Farina and Romagnosi5 developed an artificial ear and, with the help of a probe microphone placed inside it, performed measurements in order to detect differences in sound pressure levels between devices, which reached values from 60 dBA to values greater than 100 dBA (mean 90 dBA). These values, according to the researchers, are alarming, as they may endanger human hearing, and therefore it is necessary to minimize the time of use (some equipment must be used for only a few minutes a day) or reduce the volume of such equipment.
Therefore, this study aimed to determine the difference in sound pressure when young individuals use such equipment with AIEs and IEs i.e., to compare the levels of sound intensity obtained in each ear when exposed to the same input signal and to verify statistically significant differences between them. Furthermore, this study investigated the correlation between the peak intensity with the AIE and the resonance frequency of the external ear.
Material and methodsSampleThe study included 27 young individuals aged between 18 and 30 years, of whom 29.63% (8 subjects) were males and 70.37% (19 subjects) were females, with a mean age of 23 years. Individuals aged < 18 or > 30 years, or those who had any external auditory canal (EAC) impairment that could prevent the assessment were excluded from the study.
EquipmentThe study was performed using measurement equipment with probe microphone, the Hearing Aid Analyzer - Affinity® (Interacoustics). The equipment has a central unit (hardware) connected to a computer, a microphone system (one reference microphone and one probe microphone with an internal diameter of 1.8mm), a high-resolution compressor connected to a speaker, a video monitor, and a printer for recording the results.
The equipment generates, through the speaker, a signal in free field and a reference microphone ensures that the initially set level of sound pressure remains unchanged throughout the measurement. It allows the performance of the examination in the frequency range of 125-8,000Hz with a frequency resolution option of 12 or 24 steps/octave. Recorded frequency accuracy is within ± 3%. For the test, the speaker was turned off and music generated by the patient's electronic device was be used. The equipment has an intensity test range of 40-90dB SPL with accuracy of ± 1.5dB and harmonic distortion of the stimulus < 1%. The range of intensity measured with the probe microphone is 40 to 140dB SPL, with a variation of ± 2dB.
The sound device used was a Philips MP4 player®, Sony IE® (Fig. 1) and Sony AIE® (Fig. 2).


An analog caliper was used to measure the depth, in millimeters, of AIE penetration in the external ear, using the tragus as the starting point.
ProceduresThe study involved the collaboration of volunteers. First, the subjects were informed about the study and signed an informed consent. The project was presented to the research ethics committee of the institution, and approved under number 229/2008. Additionally, the project is in accordance with resolution 196/96 of the Brazilian National Health Council.
First, the external auditory canal was inspected to verify whether the participants had middle ear disorders. Then, aiming to obtain the sound pressure level of the individual portable audio equipment, measurements were performed with a probe microphone in each ear. The subjects were positioned at 40cm from the speaker at 0° azimuth. The probe microphone was introduced in the external auditory canal, to an approximate depth of insertion of 27mm from the tragus, which guaranteed the position of the probe microphone at a distance of 8mm from the tympanic membrane.
The resonance curve of the external ear canal was assessed in each subject first. With the probe microphone thus positioned, the sound pressure level curve was traced from a stimulus originating from the individual portable audio equipment of each volunteer. All subjects underwent the following order of data collection: 1) IE in the right ear, 2) IE in the left ear; 3) AIE in the right ear; 4) AIE in the left ear.
The characterization of the stimulus followed the procedure described in the study by Santos and Couto.10 To perform the measurements, a rock and roll-style song was used as stimulus. The song chosen was “I Love Rock and Roll” by ACDC. Furthermore, the equipment volume remained constant for all measurements, and 70% of the total device capacity was used.
Regarding the probe microphone measurement, it is noteworthy that the equipment used in this study to perform the measurements provided values of intensity achieved at each frequency instead of a quadratic mean of all values obtained (all tested frequencies), as it is possible to obtain with the use of other equipment available in the market. Therefore, the peak intensity and frequency values obtained in this study were used to perform the statistical correlations.
It is also worth noting that after the first measurement in each ear, the earphone was removed with care so as not to dislodge the probe microphone. Thus, the AIE was introduced and the distance from the tip of the earphone to the individual's tragus was measured with the aid of a caliper. Based on this measurement (mm) and the resonance peak obtained at the beginning of the examination, the new resonance peak of the ear was measured, as its size was reduced by the introduction of the AIE. Therefore, the formula shown in Fig. 3 was used.

After obtaining the value of the external auditory canal length, the size of the earphone obtained with the caliper was subtracted, and the formula was again applied in order to obtain the new resonance frequency.
These data were used in the statistical analysis in order to verify whether there was an association between the peak intensity obtained with the probe microphone while listening to the music and the resonance peak of the ear.
The evaluations involved in this study are described in the literature as non-invasive and painless for the patient. Such procedures are controlled by the equipment itself, in accordance with pre-established safety standards, so as not to cause injury to the auditory system.
Data analysisA quantitative and statistical evaluation of data was performed. To compare the the sound pressure level between two phones, between the ears, and between the two genders, two-way factorial analysis of variance (ANOVA) for repeated measures was used, followed by the profile test by contrasts to analyze the pressure differences between the devices and the sides, and Tukey's test was used for comparison between the genders. The variables were submitted to rank transformation due to the absence of normal distribution.
Spearman's correlation coefficient was used to assess the association between numerical variables due to the lack of normal distribution. The significance level for statistical tests was set at 5%, i.e., p < 0.05The results that showed statistically significant differences are highlighted in bold.
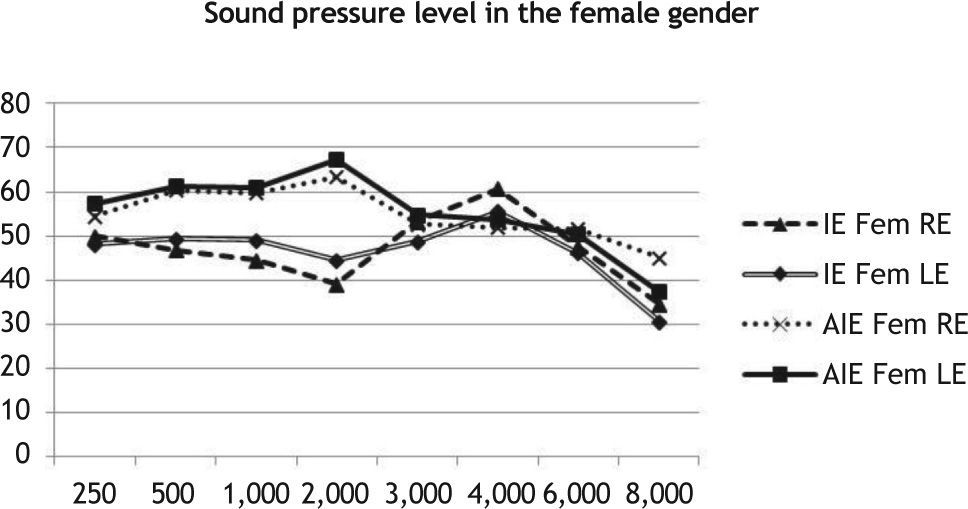
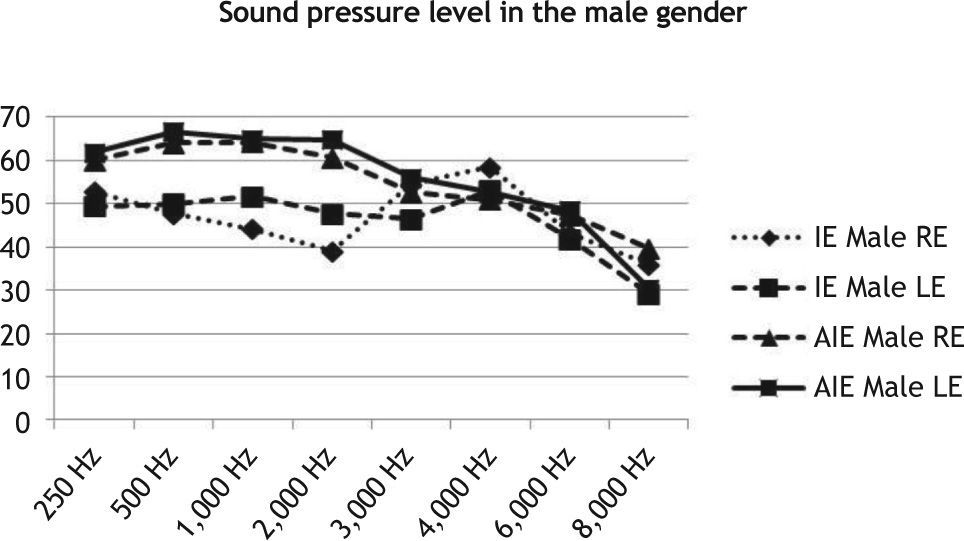
ResultsInitially, the results obtained per frequency in each gender with each of the earphones used, IE and AIE, were analyzed (Figs. 4 and 5)


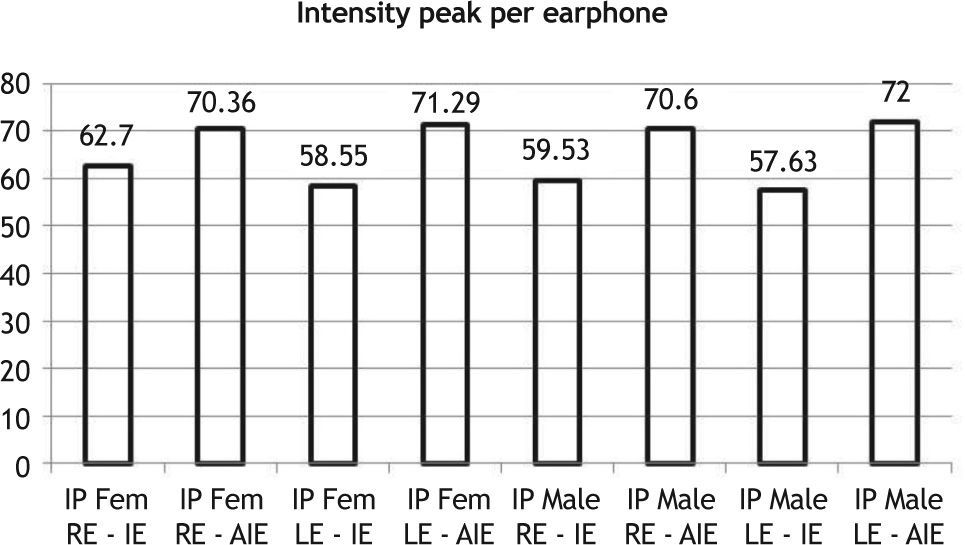
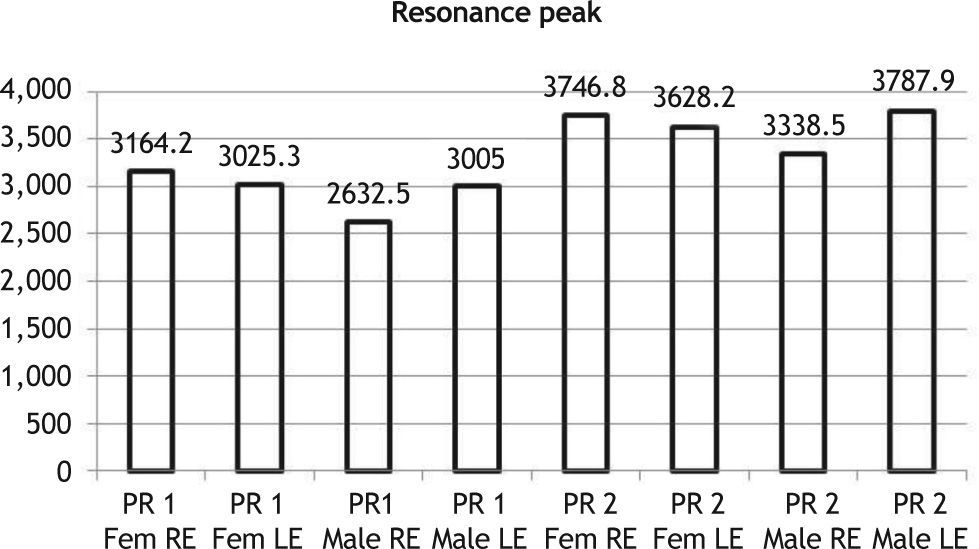
Fig. 6 presents the peak intensity obtained for each earphone. Fig. 7 shows resonance peaks obtained without the earphone and the new resonance peak calculated from the measurement of the earphone insertion in the external ear canal.


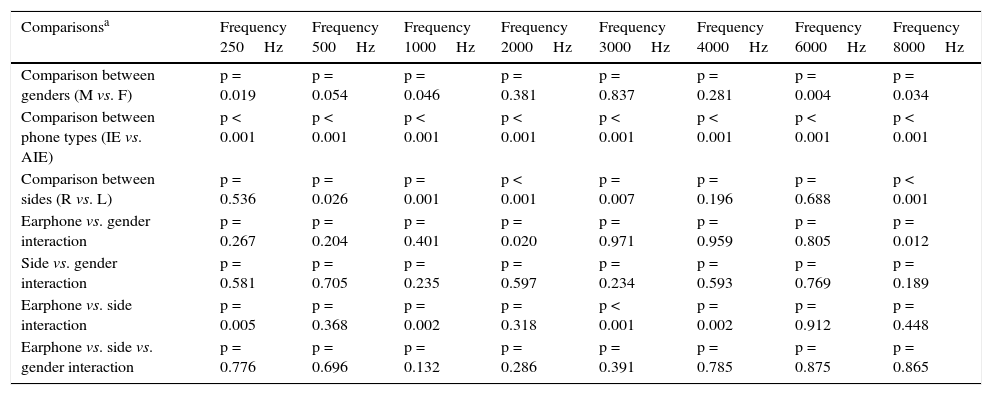
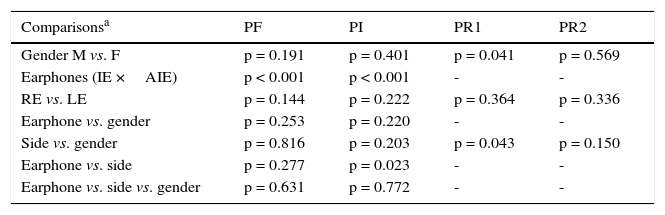
Table 1 shows the ANOVA results for repeated measures to compare the sound pressure level between the two earphones, the two ears (right and left), and the two genders. These results are given for each frequency assessed. Table 2 presents the ANOVA results for repeated measures to compare the sound pressure level between the two phones, both sides, and both genders. These results were compared with the values obtained with the peak frequency (PF), peak intensity (PI), and peak resonance obtained (PR1 and PR2).
ANOVA results for repeated measures for comparison (sound pressure level between headphones, sides, and genders) considering the tested frequencies.
| Comparisonsa | Frequency 250Hz | Frequency 500Hz | Frequency 1000Hz | Frequency 2000Hz | Frequency 3000Hz | Frequency 4000Hz | Frequency 6000Hz | Frequency 8000Hz |
|---|---|---|---|---|---|---|---|---|
| Comparison between genders (M vs. F) | p = 0.019 | p = 0.054 | p = 0.046 | p = 0.381 | p = 0.837 | p = 0.281 | p = 0.004 | p = 0.034 |
| Comparison between phone types (IE vs. AIE) | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 |
| Comparison between sides (R vs. L) | p = 0.536 | p = 0.026 | p = 0.001 | p < 0.001 | p = 0.007 | p = 0.196 | p = 0.688 | p < 0.001 |
| Earphone vs. gender interaction | p = 0.267 | p = 0.204 | p = 0.401 | p = 0.020 | p = 0.971 | p = 0.959 | p = 0.805 | p = 0.012 |
| Side vs. gender interaction | p = 0.581 | p = 0.705 | p = 0.235 | p = 0.597 | p = 0.234 | p = 0.593 | p = 0.769 | p = 0.189 |
| Earphone vs. side interaction | p = 0.005 | p = 0.368 | p = 0.002 | p = 0.318 | p < 0.001 | p = 0.002 | p = 0.912 | p = 0.448 |
| Earphone vs. side vs. gender interaction | p = 0.776 | p = 0.696 | p = 0.132 | p = 0.286 | p = 0.391 | p = 0.785 | p = 0.875 | p = 0.865 |
IE, insertion earphones; AIE, anatomical in sertion earphones; M, male gender; F, female gender; R, right ear; L, left ear.
ANOVA results for repeated measures for comparison (sound pressure level between headphones, sides, and genders) considering PF, PI, PR1, and PR2.
| Comparisonsa | PF | PI | PR1 | PR2 |
|---|---|---|---|---|
| Gender M vs. F | p = 0.191 | p = 0.401 | p = 0.041 | p = 0.569 |
| Earphones (IE ×AIE) | p < 0.001 | p < 0.001 | - | - |
| RE vs. LE | p = 0.144 | p = 0.222 | p = 0.364 | p = 0.336 |
| Earphone vs. gender | p = 0.253 | p = 0.220 | - | - |
| Side vs. gender | p = 0.816 | p = 0.203 | p = 0.043 | p = 0.150 |
| Earphone vs. side | p = 0.277 | p = 0.023 | - | - |
| Earphone vs. side vs. gender | p = 0.631 | p = 0.772 | - | - |
PF, peak resonance frequency, PI, peak resonance intensity; PR1, first measurement of peak resonance; PR2, second measurement of peak resonance; M, male; F, female; RE, right ear; LE, left ear; IE, insertion earphones; AIE, anatomical insertion earphones.
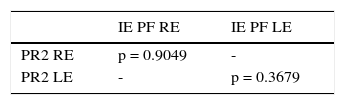
Table 3 presents the results of the correlation between peak resonance calculated from the measurement of the IE insertion in the external auditory canal and the peak frequency at which higher sound pressure level was observed.
DiscussionThe use of individual portable sound equipment has become increasingly common among young individuals, who use it with their respective earphones in numerous locations. The use of the earphone allows the individuals to listen to music without bothering those around them. Within this scenario, there has been a technological revolution in relation to earphones. Previously, the most often used type of earphones were IEs, which were made of a durable material and were one-size-fits-all, regardless of the user.
Recently, AIE phones have appeared in the market; these are made of silicone and the user can change the outer casing of the earphone, allowing an adjustment to the user's ear canal size. Due to these factors, this phone tends to penetrate more deeply into the external auditory canal, thus changing its size, and consequently, the resonance frequency of the external ear. It is worth noting that both earphones alter the resonance; however, the AIE changes the length and position of the ear canal contour, causing major changes to the external ear resonance.
The external ear, in turn, has the physiological function of amplifying the sound. One study14 has demonstrated that the broadest range of sound amplification by the outer ear without occlusion in children is on average at 2,937.56Hz, ranging between 2,180.00 and 4,407.00Hz. Mean data obtained in the present study are higher than those obtained by the abovementioned study; however, the values are within the same range (Figs. 4 and 5). It was observed that the resonance peaks obtained are, on average, 3,164.2Hz in the right ear and 3,025.3Hz in the left ear for the female gender, and 2,632.5Hz in the right ear and 3,005Hz in the left ear for the male gender.
When comparing the sound pressure levels between the IEs and AIEs, this study demonstrated that there is a statistically significant difference (Figs. 4 and 5) for both genders and both ears. The AIE had higher levels of sound pressure than the IE. This difference was observed for all frequencies, except the frequency of 4,000Hz and for the peak intensity observed.14 This fact was expected, since according to the laws of physics, when comparing the same pressure in two volumes, the former tends to be greater when the volume is smaller. Thus, the use of AIEs, which decrease the volume of the external ear, increases the sound pressure to a higher level than the observed when using IEs.
In addition to assessing the sound pressure levels, this study also evaluated the frequencies at which the highest levels of sound pressure (Figs. 6 and 7) were observed. When using IEs, the peak frequency where the highest sound pressure level occurs is around 3,000-3,600Hz. However, when performing the same measurement with the AIEs, it was observed that the peak frequency is around 1,300 to 1,700Hz. It was believed that, due to the smaller volume, the resonance peak would be more acute, which was not observed in the present study. This fact may be correlated with the frequency range of the phone itself.
Other factors may influence the results obtained, for instance, the frequency band where the earphone operates, which can influence the peak sound pressure obtained. However, it was not possible to obtain such technical data from the earphone's manufacturer. When comparing the peak frequency and intensity of both earphones, a statistically significant difference was observed.
When comparing the sound pressure levels obtained with the two phones between males and females, there was a statistically significant difference at lower frequencies (250 and 1,000Hz), demonstrating that males had a higher sound pressure level than females. A statistically significant difference in the high frequencies (6 and 8kHz) was also observed, showing that females exhibit higher sound pressure levels than males (Figs. 4 and 5).
This is mainly due to the fact that the female peak resonance is shifted more towards high frequencies than that found in males, as the length of the external auditory canal of women is shorter, making their resonance peak more acute than that of men.15
This finding regarding the difference of female and male resonance regarding the open ear was proven by ANOVA (Table 1) for the results obtained for the resonance frequency variable for each gender. Thus, this test shows that there is a difference in the resonance frequency of the ear canal between genders.
In relation to ears, when comparing the sound pressure levels obtained with different earphones, it was observed that there was a statistically significant difference for some frequencies (Table 1). In these cases, the left side always showed higher sound pressure levels than the right side. This difference does not occur when the gender variable is added to this association. One might infer that this difference could be due to the difference in ear size, and that this would be counterbalanced by the difference in size between genders. Although there is no significant anatomical difference between the two sides, studies16,17 evaluating the performance of different ears in some tests have shown that there is a difference between the two, and that the left ear always has worse results than the right ear.
When correlating the frequency at which the peak sound pressure was obtained and the new resonance frequency, a positive correlation was observed between the two. This fact may be because IEs amplify sound as a whole, rather than a specific frequency alone. Another possible explanation for this event is the sample size, i.e., it would be necessary to perform further studies with larger sample sizes in order to verify whether this correlation remains absent.
ConclusionThere was a statistically significant difference between the earphones evaluated, showing that AIEs have higher sound pressure levels than IEs for all assessed frequencies.
There was no correlation between the frequency at which the highest sound pressure levels were obtained with the AIE and the resonance peak of the closed canal. There was a statistically significant difference between ears for some tested frequencies.
Conflicts of interestThe authors declare no conflicts of interest.


