
Learning spoken and written language depends on the assimilation of acoustic elements and the representation of phonetic characteristics of a language.1 Auditory processing, phonological awareness, and auditory discrimination are factors that affect the learning of reading and writing, because they are directly related to receptive hearing.2 Researchers have associated the presence of learning disabilities with hearing deficits in children.3
After an acoustic stimulation, electrophysiological evaluation of hearing can establish an anatomical and functional correlation in the central auditory nervous system that occurs through the activation of several structures throughout the system. Thus, in cases of learning disabilities, an analysis of the integrity and function of the auditory pathways is recommended.4
Speech auditory brainstem response (Speech ABR) testing can be elicited by a wide variety of sound stimuli: click, pure tone, masked tone, and complex sounds (speech). Studies have documented the normal responses using the click stimuli in children with learning disabilities; however, recent studies suggest the presence of alterations in response to speech stimuli, due to the existence of subcortical deficits associated with learning disorders.5–7
Case reportThe subjects selected for this study were individuals with scholastic difficulties with a discrepancy between ability and academic performance. The diagnosis was based on a long and detailed study carried out by a multidisciplinary team, consisting of a psychologist, speech therapist, educational psychologist, physical therapist, psychomotrician, neurologist, and psychiatrist of the Research Laboratory of Learning Disorders, Disabilities, and Attention Deficit Disorder of the Faculdade de Ciências Médicas (Laboratório de Pesquisa em Distúrbios, Dificuldades de Aprendizagem e Transtorno de Atenção da Faculdade de Ciências Médicas – DISAPRE) of the Universidade Estadual de Campinas (UNICAMP), Campinas, São Paulo, Brazil. The diagnosis was finalized after ruling out genetic, organic, psychological, and psychiatric disorders that could cause those alterations. The present study reports two male cases (10 and 11 years old) who were assessed for a Master Degree's dissertation. The parents/guardians were informed of the study goals and signed the free and informed consent form No. 431,184/2013.
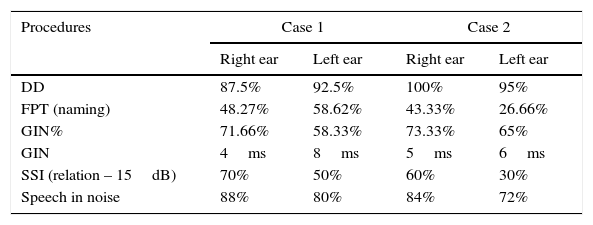
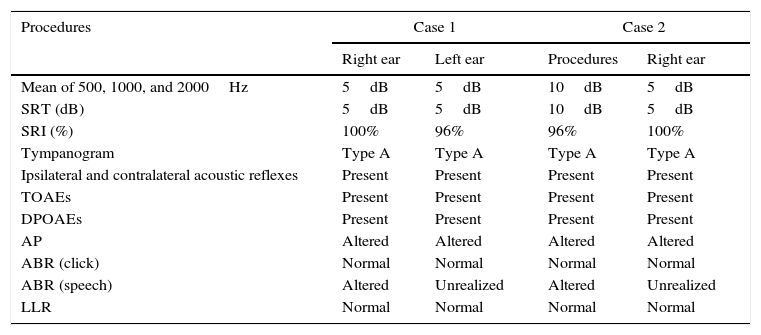
A basic audiological evaluation was performed and the results were within the normal range, bilaterally. At the behavioral assessment of auditory processing (AP), an alteration was identified in the auditory abilities of figure-ground for verbal sounds, temporal ordering, and temporal resolution (Table 1), whereas at the AP electrophysiological evaluation, the responses were within the normal range in the ABR (click) and long latency responses (LLR; Table 2) were observed. The results of transient otoacoustic emissions (TOAEs) and distortion product otoacoustic emissions (DPOAEs) were normal bilaterally.
Assessment values of auditory processing.
| Procedures | Case 1 | Case 2 | ||
|---|---|---|---|---|
| Right ear | Left ear | Right ear | Left ear | |
| DD | 87.5% | 92.5% | 100% | 95% |
| FPT (naming) | 48.27% | 58.62% | 43.33% | 26.66% |
| GIN% | 71.66% | 58.33% | 73.33% | 65% |
| GIN | 4ms | 8ms | 5ms | 6ms |
| SSI (relation – 15dB) | 70% | 50% | 60% | 30% |
| Speech in noise | 88% | 80% | 84% | 72% |
DD, Dichotic Digits test; FPT, Frequency Pattern Test; GIN, gap in noise; GIN%, gap in noise (%); SSI, synthetic sentence identification test with ipsilateral competing message.
Values of the performed hearing assessments.
| Procedures | Case 1 | Case 2 | ||
|---|---|---|---|---|
| Right ear | Left ear | Procedures | Right ear | |
| Mean of 500, 1000, and 2000Hz | 5dB | 5dB | 10dB | 5dB |
| SRT (dB) | 5dB | 5dB | 10dB | 5dB |
| SRI (%) | 100% | 96% | 96% | 100% |
| Tympanogram | Type A | Type A | Type A | Type A |
| Ipsilateral and contralateral acoustic reflexes | Present | Present | Present | Present |
| TOAEs | Present | Present | Present | Present |
| DPOAEs | Present | Present | Present | Present |
| AP | Altered | Altered | Altered | Altered |
| ABR (click) | Normal | Normal | Normal | Normal |
| ABR (speech) | Altered | Unrealized | Altered | Unrealized |
| LLR | Normal | Normal | Normal | Normal |
SRT, speech recognition threshold; SRI, speech recognition index; TOAEs, transient otoacoustic emissions; DPOAEs, distortion product otoacoustic emissions; AP, auditory processing; ABR, auditory brainstem response; LLR, long latency responses.
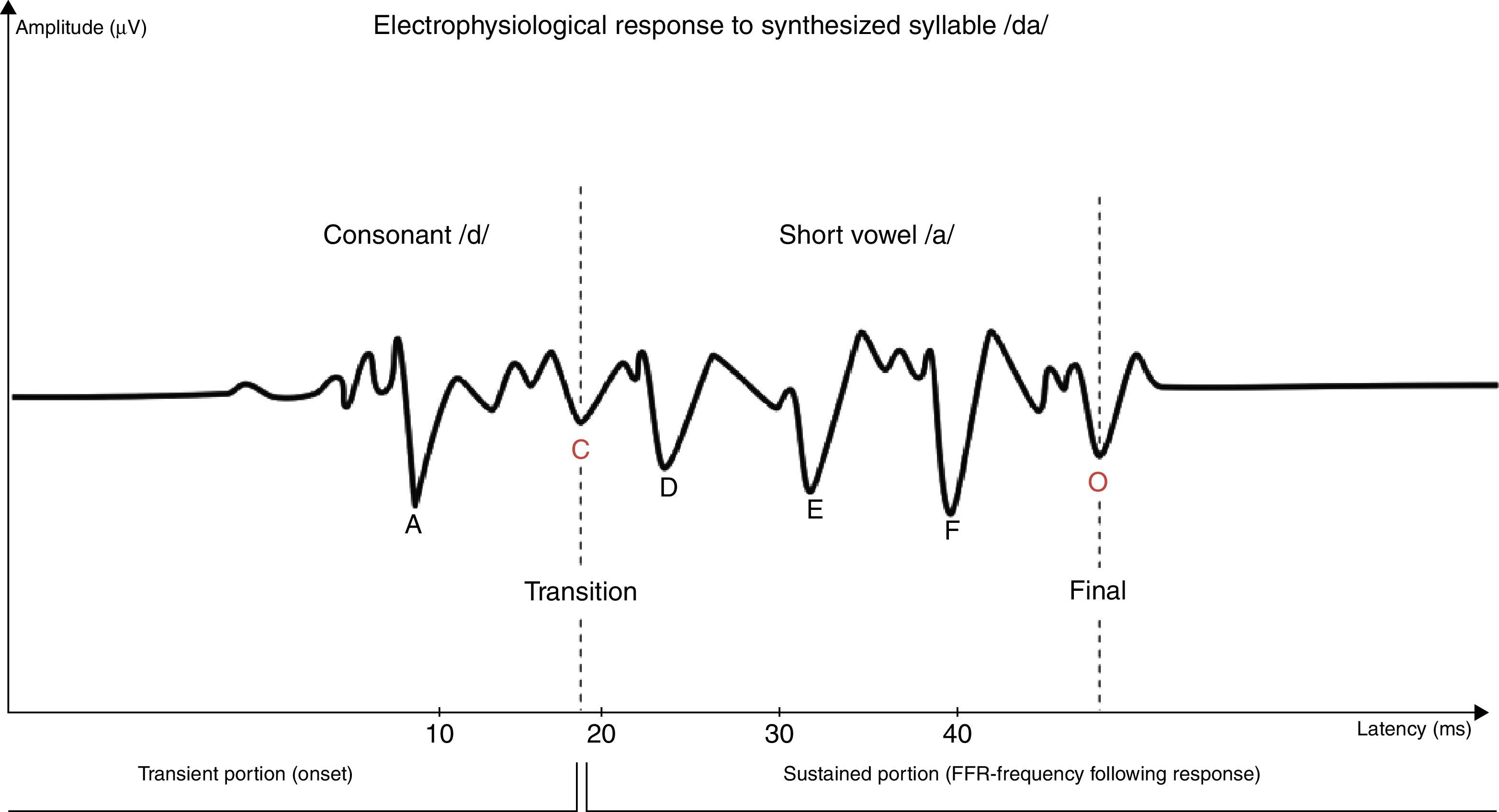
ABR with speech stimuli was carried out with the synthesized syllable /da/, at a rate of 10.9 stimuli per second, provided by the BioMARK™ software of the Biologic device. A total of 6000 stimuli were given in two bursts of 3000, and the analysis was performed on the sum of the tracing. The stimuli were applied through an insertion phone in the right ear at 80 SPL (sound pressure level), because of the known superiority of the left hemisphere for speech processing.8
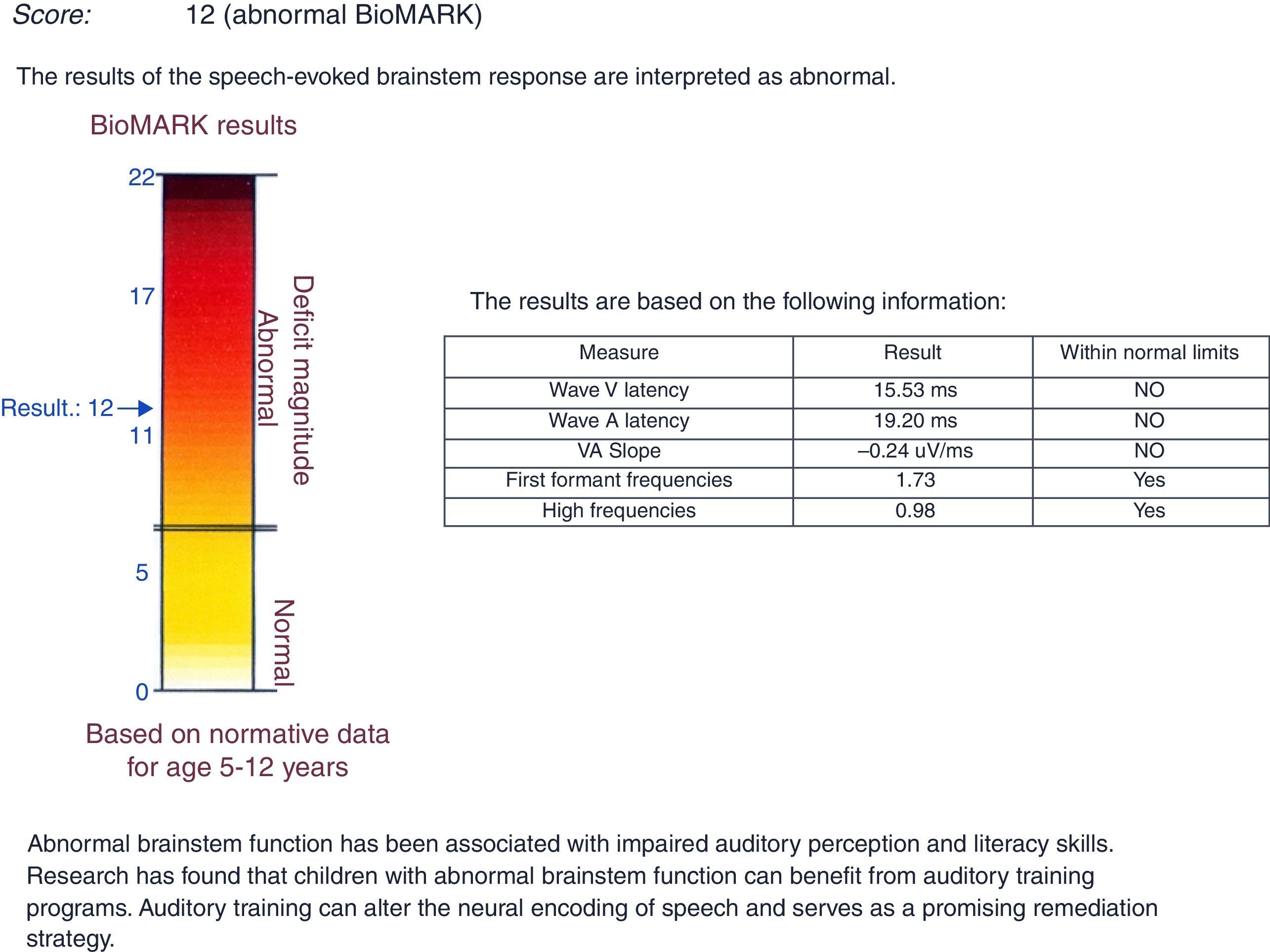
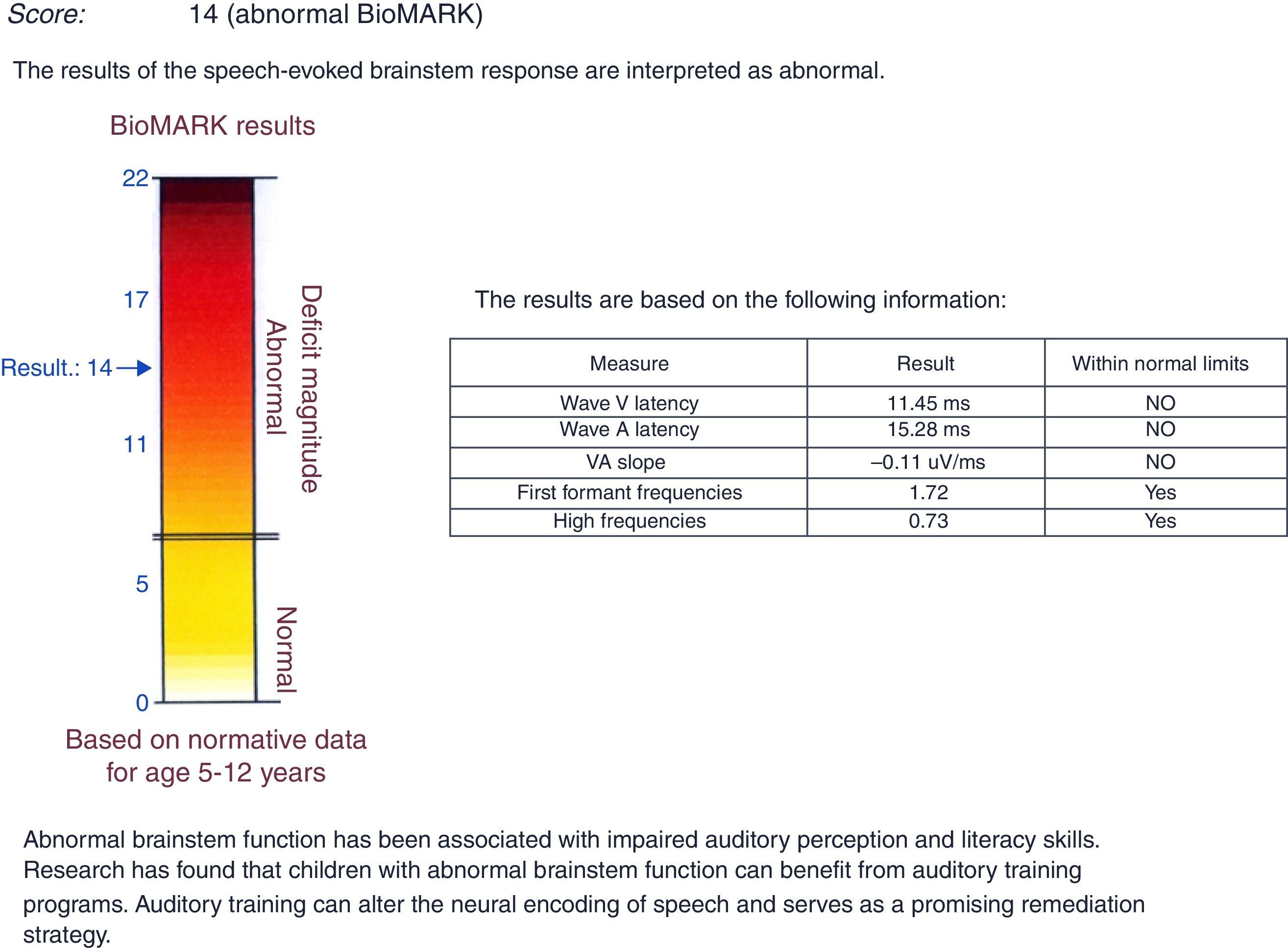
The stimulus consisted of the consonant /d/ (transient portion – onset) and a short vowel /a/ (sustained portion – frequency following response). The C waveform represents the transition between consonant and vowel, whereas the O wave represents the end of the vowel (Fig. 1). After the collection, the latency and amplitude of the transient portion (V and A waves) and the VA slope (VA amplitude/VA duration) were analyzed using the normative BioMARK™ wave as the basis for analysis. In both cases, abnormal responses were observed in the latency values of the waves V, A, and VA slope (Figs. 2 and 3).

.")
 with speech stimulus and abnormal responses. Researcher's data from a male patient (11 years old).")
In the analysis of the results, ABR with click stimulus were normal in both cases, in agreement with studies in the literature that indicate that only the processes involved in encoding speech signals in the brainstem region are altered in children with learning disabilities. These results show that the ABR with click and speech stimuli differ in how they stimulate the auditory structures along the central auditory nervous system (CANS), as the different acoustic stimuli reflect distinct neural process.5,7
In the analysis of ABR with speech stimuli, abnormalities were observed in both cases, with significantly prolonged absolute latency values of V and A waves, as well as of the VA slope. Studies support these findings and describe a difference between the V and A wave latency values in children with learning disabilities when compared to children with normal development. This suggests a rethinking of how speech sounds are encoded and the functional role of the structures responsible for generating these waves (the region of the lateral lemniscus and inferior colliculus).5–7
The findings of this study suggest the existence of functional impairment in speech processing in the brainstem region, identified by prolonged latencies of V and A waves and VA slope, suggesting that the physiological mechanisms are altered, even without a proven neurobiological abnormality in patients exhibiting scholastic difficulties. As a result of this deficit in speech perception, there is an impairment of the communication and language processes, with consequent degradation of linguistic and paralinguistic information that causes difficulties in academic skills. This can result in severe consequences in quality of life and social interactions and culminate in learning disorders. Thus, there is a negative impact on the processing of fast acoustic signals in the specialized cortical structures, which do not respond to the sound stimulus in a synchronous and organized fashion and thus render the interpretation and understanding of the meaning difficult for children with scholastic difficulties.
Several abnormalities in sound processing can be observed in patients with learning disabilities. Thus different levels of the auditory trajectory should be investigated to establish a differential diagnosis. One way to evaluate the CANS is through behavioral tests; however, the evaluation is time-consuming and requires effective patient participation. For patients with learning difficulties, ABR with speech stimulus is indicated, since it is an objective, practical, and effective test that does not depend on the patient's response and is independent of attention; additionally, it provides an analysis of numerical measures that can be used as a predictor of the degree of the disorder.
According to Chandrasekaran and Kraus,9 the analysis of absolute latency values for ABR with speech stimuli can help differentiate and establish different clinical pictures, and allow for an objective measure of subcortical speech processing. This analysis would be very important in cases of learning disabilities that include several other subgroups of disorders, including scholastic difficulties. Researchers stress that this procedure can be used to evaluate auditory function and provide additional information in the diagnosis of learning disabilities and auditory processing disorders.10
The present findings suggest that changes in the perception and processing of auditory information observed in children with scholastic difficulties appear to be the same as those seen in children with learning disabilities. Thus, the authors stress the importance of evaluating children with scholastic difficulties, considering that alterations in speech sound processing appear to be of crucial importance in the learning process. Knowing the magnitude of hearing alterations in these patients may suggest more aggressive actions for the prevention, detection, and treatment of this disorder.
ConclusionAnalysis of these two cases showed the value of using ABR with speech stimuli in the evaluation of children with scholastic difficulties, considering the abnormalities detected in this study. This procedure is objective, fast, and effective. It does not require the patient's conscious participation and provides numerical data that can demonstrate the CANS maturation and, therefore, can function as a biomarker of scholastic difficulties.
The ABR study with speech stimuli is very promising. Further studies with more subjects, would be important to monitor and demonstrate these alterations. Additionally, longitudinal follow-up of these cases would be interesting to assess test accuracy and treatment effectiveness, as well as to investigate and monitor the consequences of impaired speech perception in cases of scholastic difficulties.
FundingThis study was funded by FAPESP.
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Sanfins MD, Borges LR, Ubiali T, Colella-Santos MF. Speech-evoked auditory brainstem response in the differential diagnosis of scholastic difficulties. Braz J Otorhinolaryngol. 2017;83:112–6.
Peer Review under the responsibility of Associação Brasileira de Otorrinolaringologia e Cirurgia Cérvico-Facial.
gology is pleased to honor the reviewers


