
Hemotympanum occurs in several conditions, including temporal bone fracture, therapeutic nasal packing, epistaxis, anticoagulant therapy, and blood disorders. Glanzmann's thrombasthenia, a rare congenital bleeding disorder, represents an infrequent cause of hemotympanum. This report presents a case of bilateral spontaneous hemotympanum in Glanzmann's thrombasthenia.
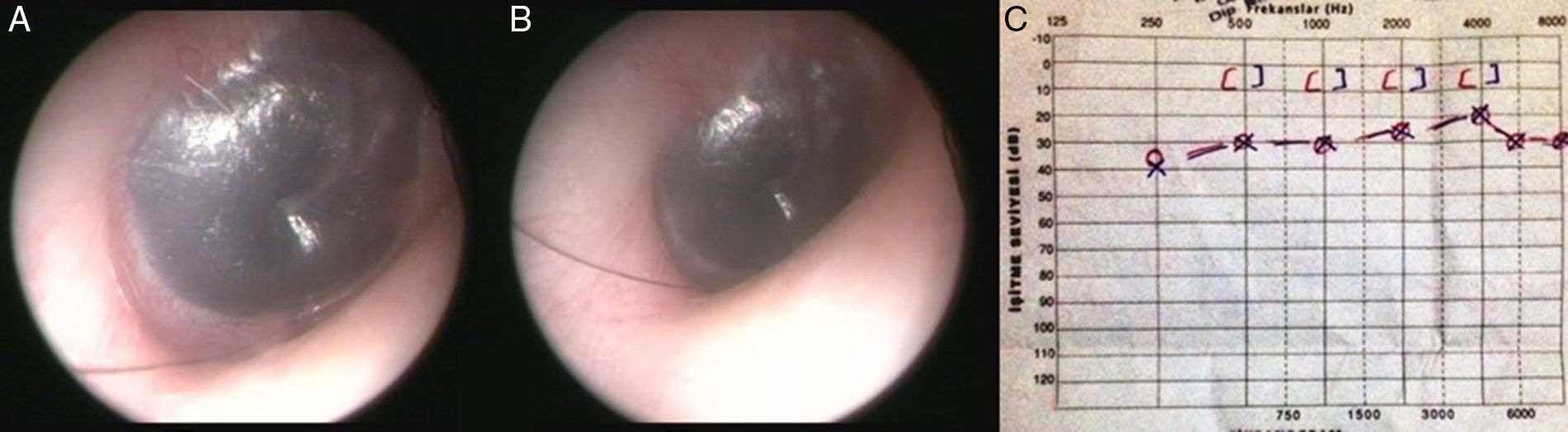
Case presentationA 12-year-old male presented with a two-day history of progressive bilateral hearing loss. The patient was previously diagnosed with type 2 Glanzmann's thrombasthenia, due to prolonged bleeding following circumcision in 2003. Otolaryngological examination of the ear, using microscopy, revealed the presence of bilateral hemotympanum (Fig. 1A and B). Other examination results were unremarkable. The patient's history was clear from trauma, barotrauma, chronic otitis media, or anticoagulant therapy. An audiogram revealed symmetrical, bilateral conductive hearing loss (Fig. 1C). Tympanometry revealed flat bilateral tympanograms (Tip B). Acoustic reflexes were absent both ipsilaterally and contralaterally. Computerized tomography (CT) was not used because of a short medical history, and because of concerns regarding the side effects of radiation. The patient's platelet count was 200,000/mm3; bleeding time was 10min (normal range: 1–3min). All other hematological test results were unremarkable. The patient was diagnosed with bilateral spontaneous hemotympanum. There is a high rate of spontaneous resolution of hemotympanum, but considering the immediate impacts of hemotympanum on a child's hearing, amoxicillin/clavulanic acid (40mg/kg/day, 2×1) was prescribed for two weeks in combination with nasal decongestant (three per day, 3×1). The tympanic membrane was reassessed after medical therapy. The tympanic membrane was normal and mobile during the Valsalva maneuver. The audiogram, acoustic emittance, and temporal magnetic resonance imaging (MRI) results were normal, including at the ng otolaryngological examination.
 Microscopic view of the right tympanic membrane. (b) Microscopic view of the left tympanic membrane. (c) Audiogram of the patient demonstrating bilateral conductive hearing loss.")
Written informed consent was obtained from the patient who participated in this case.
DiscussionHemotympanum, characterized by the accumulation of blood in the middle ear and diagnosed using otoscopy, manifests with partial or total occupancy of the tympanic membrane by a bright red or dark blue color.1 The presence of blood in the tympanic cavity can cause conductive or mixed hearing loss.1 Patients typically complain of acute-onset hearing loss in the affected ear. In general, otalgia and aural fullness present concomitantly.1
Traumatic temporal bone fractures are the most frequently reported causes of hemotympanum.2 Other antecedents include therapeutic nasal packing, epistaxis, chronic otitis media with effusion, blood diseases, and the use of anticoagulants.3
Coagulation defects represent the other cause of hemotympanum.4,5 In the present case, Glanzmann's thrombasthenia was of type 2. This is the first report of spontaneous bilateral hemotympanum in Glanzmann's thrombasthenia, a rare congenital bleeding disease. Platelet aggregation defects occur in Glanzmann's thrombasthenia, in which the platelet surface glycoproteins Gp2b and Gp3a can exhibit abnormalities or defects. The genes encoding for Gp2b and Gb3a localize to chromosome 17q 21-23; any mutations can lead to platelet dysfunction. In Glanzmann's thrombasthenia, platelet morphology and count are normal, but prolonged bleeding times are typically observed. Glanzmann's thrombasthenia is divided into three types. The classification of types 1 and 2 is based upon the amount of Gp2b/Gp3a present. However, in type 3, the amount of Gp2b/Gp3a is normal even with abnormal function. There is no known cure for Glanzmann's thrombasthenia. Supportive treatment and platelet transfusion during bleeding represent the most effective therapeutic approaches. In rare cases, bone marrow transplants have been performed successfully. Glanzmann's thrombasthenia has a very good prognosis with appropriate care.5
Hemotympanum is self-limiting condition early realize and medical therapy correct hearing disability rapidly. Antibiotherapy and local and systemic anticongestants can be used. However, other researchers have suggested the use of myringotomy, and the application of tubes during persistent hearing loss.4
In summary, many factors can cause hemotympanum. Hematological diseases should be considered in the differential diagnosis. Considering the immediate impacts of hemotympanum on a child's hearing, early realize and conservative medical therapy may prevent long-term sequelae of persistent hemotympanum.
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Yazici ZM, Çelik M, Yegin Y, Güneş S, Kayhan FT. Glanzmann's trombastenia: um caso raro de hemotimpanum bilateral espontânea. Braz J Otorhinolaryngol. 2015;81:224–5.
Institution: Bakirkoy Dr. Sadi Konuk Training and Research Hospital, Istanbul, Turkey.
gology is pleased to honor the reviewers


