
Laryngeal involvement by cartilaginous tumors is rare. However, although accounting for only 1% of laryngeal tumor pathology, they are the most frequently occurring non-epithelial neoplasms. The most probable location is the endolaryngeal surface of the cricoid cartilage. Their symptoms are variable, depending on the size and location, and may include hoarseness, stridor, and dyspnea. Treatment is based on surgical excision. Some centers take into account the degree of differentiation and whether it is a case of relapse when deciding to perform a radical resection.
AimTo evaluate this disease in a sample of the Portuguese population.
MethodsA review of the medical records from 2002 to 2012 by assessment of clinical processes was performed. Data on demographics, clinical treatments, and outcomes were collected.
ResultsSix patients were included in the study. Five of them underwent total laryngectomy, and in one case, partial excision of the thyroid cartilage was performed. None of the patients had either metastases or tumor-related death.
ConclusionLaryngeal chondrosarcomas remain a rare disease of unknown etiology, with slow and insidious symptoms. The treatment is surgical, with favorable prognosis, and metastases rarely occur. The main concern regards their propensity to relapse.
O acometimento laríngeo por tumores cartilaginosos é raro. No entanto, apesar de representarem 1% da patologia tumoral laríngea, são as neoplasias não epiteliais mais frequentes. Localizam-se mais frequentemente na face endolaríngea da cartilagem cricóide. Tem sintomatologia variável consoante o tamanho e a localização, podendo incluir disfonia, estridor e dispneia. O tratamento é essencialmente cirúrgico. Alguns centros levam em conta o grau de diferenciação e de se tratar ou não de recidiva, quando da decisão de ressecção mais ou menos radical.
ObjetivoAvaliar esta patologia numa amostra da população portuguesa.
MétodoRevisão da casuística no intervalo de tempo 2002-2012, através de consulta dos processos clínicos. Foram coligidos os dados demográficos e clínicos relevantes, os tratamentos efetuados e os resultados.
ResultadosForam incluídos seis pacientes. Cinco foram submetidos à laringectomia total e um foi submetido à excisão da asa esquerda da cartilagem tiroide. Nenhum apresentou metástases ou morte relacionada com o tumor.
ConclusãoOs condrossarcomas laríngeos permanecem como patologia rara, de etiologia desconhecida, com crescimento lento e clínica insidiosa. O tratamento é cirúrgico, com prognóstico favorável, com a metastização a ocorrer raramente. A maior preocupação decorre da sua propensão à recidiva.
Rare and insidious pathological entities require extra attention for their appropriate diagnosis and treatment. Laryngeal involvement by cartilaginous tumors is rare.1–4 However, despite representing only 1% of laryngeal tumor pathology, they are the most frequently occurring non-epithelial neoplasms.2 Chondromas are the most common benign tumors, most often affecting the cricoid cartilage (75%).3 Only approximately 0.1% of cartilaginous tumors are chondrosarcomas, which are most commonly low grade.1,2,5
Chondrosarcoma is a slow-growing malignant tumor, most commonly located in the pelvis, femur, ribcage, humerus, scapula, fibula, sacrum, and sternum. More rarely, it is found in the head and neck, in approximately 10–20% of the total number of cases.2,5 In the larynxchondromas they are located in most cases in the endolaryngeal surface of the posterior portion of the cricoid cartilage.1,2,5,6 It less often affects the arytenoid cartilage or the thyroid cartilage in the inferior border of its laryngeal surface.5,7
Its etiology remains unknown, but there are some hypotheses regarding the contribution of medullary-cervical trauma and vertebral instability,3 repeated laryngeal trauma,5 radiotherapy, Teflon® injection,6 and irregular ossification of laryngeal cartilage.7
As for the epidemiological characteristics, it is most often observed in adult patients in the sixth and seventh decades of life,1 although it can be found at any age. It affects more males than females, at a ratio of 3:1.3 Cartilaginous tumors with higher degrees of malignancy are found at older ages.6
Symptoms are variable and depend on tumor size and location. Tumors may be asymptomatic while small, and their growth can trigger dysphonia, stridor, dyspnea, and dysphagia. The clinical picture very rarely includes pain.1,3,5 There have been cases described with concurrent vocal cord paralysis, which is thought to originate from cricoarytenoid joint fixation and not the recurrent laryngeal nerve lesion.1
Endoscopic assessment must be considered, taking into account the tumor's common subglottic location. The clinician must search for submucosal bulging, usually with regular mucosa and in a more posterior location, which is small-sized (usually smaller than 3–4cm).5 Vocal cord immobilization can be found.
During imaging assessment and in the presence of larger masses, an anterior displacement of the larynx in the lateral cervical radiograph can be observed. However, its clinical suspicion requires the performance of computed tomography (CT) or magnetic resonance imaging (MRI). Some authors suggest that CT is the imaging examination of choice,1–3,8 disclosing a hypodense, well-defined image with calcifications inside, cartilage destruction, and structure distortion.9
Others report the superiority of MRI due to its greater accuracy in distinguishing between tumor and other paralaryngeal tissues.5,8 The signal strength is low on T1 and high on T2, with a characteristic mosaic pattern.8 The F-18 fluorodeoxyglucose-positron emission tomography (FDG-PET) is helpful in tumor grading, metastasis detection, and local recurrence assessment. The uptake value of 1.3 was set as the limit between benign and malignant lesions, with the higher uptake showing greater differentiation.8,10
In spite of clinical suspicion and the above-mentioned complementary diagnostic tests, the diagnosis can only be definitely established by histological study. Often, this can only be correctly achieved through the study of the surgical specimen, as endoscopy biopsies may be inconclusive due to the difficulty of handling a submucosal pathology.1,5
Histological analysis discloses hyaline cartilage, with giant cartilage cells, pleomorphism, and hyperchromatic nuclei. The differential diagnosis is made with chondroma, fibrosarcoma, osteosarcoma, and chondromyxoid fibroma. According to the cell differentiation degree on histopathological findings (mitotic index, cellularity, and nuclear size), laryngeal chondrosarcoma is graded according to the classification proposed in 1943 by Jaffe and Lichtenstein for chondrosarcomas of long bones and updated in 1977 by Evans et al., sub-divided into three grades (I–III).
Most authors reported difficulty in differentiating low-grade chondrosarcomas (I) from chondromas (benign tumors) due to the absence of mitotic activity, presence of small nuclei, chondroid intercellular space, and frequent calcifications. Lesion size can help in the differentiation, because the chondroma is usually smaller than the chondrosarcoma. The diagnosis becomes easier in grade II due to the presence of larger nuclei, myxoid intercellular space, and low mitotic index; and in grade III, due to higher mitotic index and nuclear atypia.2,5,6
Laryngeal chondrosarcomas are less aggressive in the larynx than in other locations; they are slow-growth tumors, more commonly diagnosed in the early stages of differentiation. Moreover, metastases rarely occur (8.5%)5; when they occur, they are more often found in the lungs and skeleton.
The treatment is based mainly on surgical excision, which can be achieved endoscopically or by open technique.1
Endoscopic treatment is usually limited to smaller lesions. The use of laser therapy allows for a better control of bleeding, and three types can be used. The CO2 laser is more indicated for cases involving stenosis. The potassium-titanyl-phosphate (KTP) laser is absorbed by hemoglobin, provides good electrocoagulation, and does not penetrate deeply into tissues. It is more useful in cases of lesions encroaching into the lumen. The neodymium-doped yttrium aluminum garnet (Nd:YAG) laser is absorbed by tissues, allowing for an appropriate deeper resection, even in the presence of ossification.11 When performing the conventional technique, the clinician can be more or less radical, with some centers taking into account the degree of differentiation and whether or not to treat recurrence. In cases of advanced lesions, in which total lesion removal is unlikely, or when there is infiltration of surrounding tissues or an advanced degree of differentiation/malignancy, or in cases of recurrence, total laryngectomy should be performed.1,5,10
Due to its low radiosensitivity, the role of radiotherapy is controversial, and is not part of the first-line treatment. It is reserved for cases of recurrence, extensive and aggressive lesions, or even inoperable ones.1,2,5 Chemotherapy is not widely employed due to the rare occurrence of metastases.2,5
Most authors report a tendency to recur in about 35–40% of cases.2 This entity usually has good prognosis, with a survival rate of 95% at ten years, although lesion size, degree of differentiation, and whether a radical surgical procedure was performed should be taken into account.1,2 The follow-up is necessarily long, lasting over five years due to the tendency of late recurrence.7
Materials and methodsThe present study involves a review of chondrosarcoma cases from 2002 to 2012, through the review of clinical processes. Demographics and relevant data on clinical characteristics, treatments performed, and outcomes were collected.
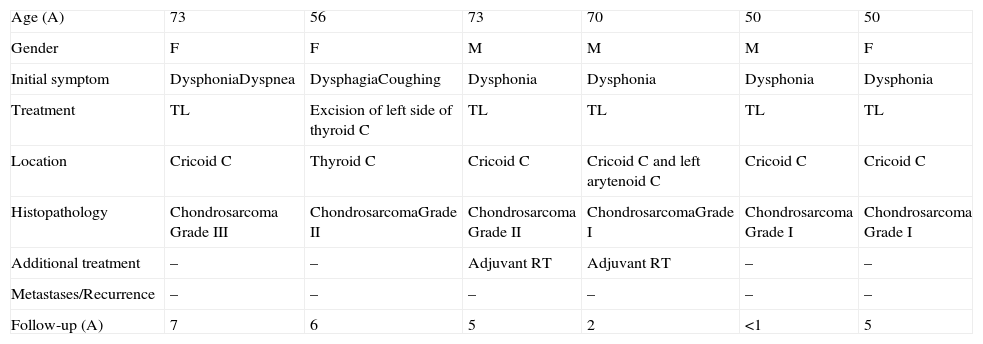
ResultsSix patients were included in the study, three males and three females (Table 1). The mean age at diagnosis was 62 years, ranging from 50 to 73 years. The most common symptom was dysphonia (for more than one year). Total laryngectomy was performed in five patients, and one patient was submitted to excision of the left portion of the thyroid cartilage. Radiotherapy was used as adjuvant therapy in two cases. The histological analysis showed three grade I chondrosarcomas, two grade II, and one grade III. The most frequent location was the cricoid cartilage. In this series, there were no patients with metastases or whose death was tumor-related. The mean follow-up was 4.16 years, ranging from zero to seven years.
Summary of case series: patients with laryngeal chondrosarcoma (2002–2012).
| Age (A) | 73 | 56 | 73 | 70 | 50 | 50 |
| Gender | F | F | M | M | M | F |
| Initial symptom | DysphoniaDyspnea | DysphagiaCoughing | Dysphonia | Dysphonia | Dysphonia | Dysphonia |
| Treatment | TL | Excision of left side of thyroid C | TL | TL | TL | TL |
| Location | Cricoid C | Thyroid C | Cricoid C | Cricoid C and left arytenoid C | Cricoid C | Cricoid C |
| Histopathology | Chondrosarcoma Grade III | ChondrosarcomaGrade II | Chondrosarcoma Grade II | ChondrosarcomaGrade I | Chondrosarcoma Grade I | Chondrosarcoma Grade I |
| Additional treatment | – | – | Adjuvant RT | Adjuvant RT | – | – |
| Metastases/Recurrence | – | – | – | – | – | – |
| Follow-up (A) | 7 | 6 | 5 | 2 | <1 | 5 |
Age (A – years), considered at the time of diagnosis; M, male; F, female; TL, total laryngectomy; C, cartilage; RT, radiotherapy.
Laryngeal chondrosarcoma is a rare disorder of unknown etiology, with slow growth and insidious clinical picture. The occurrence of distant metastases is rare. A high degree of suspicion is required for early detection. Treatment is based on surgical excision, with a favorable prognosis. Although rarely possible, considering the usual location of these tumors in the posterior surface of the cricoid cartilage, laryngeal function should be preserved. The main concern regarding these tumors is their propensity to relapse, which usually occurs at a later stage, making long-term surveillance mandatory.
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Oliveira JF, Branquinho FA, Monteiro AR, Portugal ME, Guimarães AM. Laryngeal chondrosarcoma – Ten years of experience. Braz J Otorhinolaryngol. 2014;80:354–8.


